
 Overview
Overview
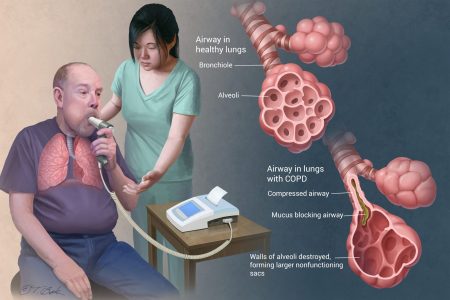
Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, mucus (sputum) production and wheezing. It’s caused by long-term exposure to irritating gases or particulate matter, most often from cigarette smoke. People with COPD are at increased risk of developing heart disease, lung cancer and a variety of other conditions.
Emphysema and chronic bronchitis are the two most common conditions that contribute to COPD. Chronic bronchitis is inflammation of the lining of the bronchial tubes, which carry air to and from the air sacs (alveoli) of the lungs. It’s characterized by daily cough and mucus (sputum) production.
Emphysema is a condition in which the alveoli at the end of the smallest air passages (bronchioles) of the lungs are destroyed as a result of damaging exposure to cigarette smoke and other irritating gases and particulate matter.
COPD is treatable. With proper homoeopathic management, most people with COPD can achieve good symptom control and quality of life, as well as reduced risk of other associated conditions.
Complications
COPD can cause many complications, including:
Respiratory infections:
People with COPD are more likely to catch colds, the flu and pneumonia. Any respiratory infection can make it much more difficult to breathe and could cause further damage to lung tissue. An annual flu vaccination and regular vaccination against pneumococcal pneumonia can prevent some infections.
Skeletal Muscle weakness and cachexia
Skeletal muscle weakness, loss of fat free mass, general cachexia are all consequences of COPD. Decreased exercise capacity due to dyspnoea leads to inactivity which potentiates inflammation and muscle weakness. Enhanced oxidative stress in COPD, reduced anti oxidant capacity and enhanced nitrosative stress are also mechanisms that potentiate protein degradation and muscle atrophy. An acute exacerbation further decreases the exercise capacity by increasing the inflammation and by the associated inactivity.
Screening test: Measuring exercise capacity by a simple 6 Minute Walk Distance Test
Treatment: Pulmonary rehabilitation and exercise training or even simple walking, improves exercise capacity. Exercise training not only breaks the viscious cycle of inactivity, increased systemic inflammation and enhanced muscle atrophy but it also has been shown to improve the oxidative enzymes in the mitochondria of skeletal muscles.
Cardiovascular diseases:
Diseases of the heart and the lungs are closely associated with each other and dysfunction of one organ can impact the other. In COPD this association can either due to similar risk factors like cigarette smoke, coronary artery disease, or congestive heart failure and COPD or could be due to cardiac implications of primary lung disease like secondary pulmonary hypertension and ventricular dysfunction due to increased intra-thoracic mechanical load.
Diagnosis of co existing cardiovascular morbidity: It is important that we screen all patients with COPD for presence of Coronary Artery Disease and cardiac function. The vice versa is also true and patients with atherosclerotic heart disease should be investigated for the concomitant presence of airflow obstruction. An electrocardiogram and a 2 D echocardiography with special emphasis on right heart imaging should be done for all COPD patients. Cardiac MRI where possible will pick up covert heart failure. Plasma NAtriuretic Peptides (BNP) is important to identify presence of heart failure in COPD patients especially in an acute exacerbation.
Management of coexisting COPD and Cardiac Disease:
Digitalis. [Dig]
Digitalis is known chiefly for its action on the heart, and it is rare that a patient suffering from an affection of that organ does not get Digitalis in some form. There is no doubt but that it is a much abused drug and when used in strong doses its action is cumulative and dangerous. Its symptoms are, however, clear, and briefly stated, as follows: The pulse is slow, but primarily strong, there is great weakness of the cardiac tissue, and, secondarily, the pulse becomes weak. Extra exertion increases its rapidity, but diminishes its force, so that the quick pulse becomes irregular and intermittent. This irregular intermittency is a marked symptom. The heart feels as if the blood stood still.
There is weakness and numbness of the left arm, and often blueness of the surface of the body, or cyanosis. The patient fears that the heart will stop beating if he should make any motion. This uneasy feeling about the chest rarely amounts to real pain. Gelsemium has the opposite symptom to this. The patient is roused out of sleep feeling that the heart will stop beating, and he is impelled to move about to keep it going. A number of drugs have numbness of the left arm in heart affections, notably Aconite, Kalmia, Rhus and Pulsatilla. These are not “keynote ” symptoms, however, as is shown further on. The Digitalis patient has a doughy look to the skin; there is often a sick feeling at the stomach after eating. Apis has a symptom that will lead to its use in heart affections, namely: “He does not see how he can get another breath.” In pericarditis with effusion it is one of our best remedies vieing here with Cantharis, but the latter has burning and spasms. Cartier recommends the 30th or 200th. Like Arsenicum and Lachesis, the tendency of Digitalis is downwards, and it must be used cautiously and only when indicated homoeopathically. There are numerous other symptoms that will indicate Digitalis. Disturbed sleep, apprehensiveness, deep sighing, slow respiration,, dry cough, suffocative spells; in fact, such symptoms as may be caused by an irregular distribution of the blood. Digitalis is also indicated in dropsical conditions dependent on heart trouble, swelling of feet and ankles, anasarca, cardiac dropsy associated with slow pulse, urine suppressed or scanty. Apocynum is similar in this relation. The special field of usefulness of Digitalis is inflammation of the heart muscle approaching insidiously and in sudden cases of myo-or endo-carditis with the symptoms above outlined. The first noticeable benefit is a steadier heart’s action and an increased flow of urine. To use it in strong doses for a long time will render the patient incurable.
Cactus grandiflorus. [Cact]
Perhaps the next most important remedy in heart affections,from the homoeopathist’s standpoint, is Cactus. Its well known characteristic symptom, “Sensation as if the heart were grasped with an iron hand,” which clutches and relaxes alternately, is ever present to the mind. It should be borne in mind that not all patients express themselves alike. A squeezed sensation may mean the same symptom. It has, however, other symptoms. It is similar to Arnica in chest soreness and constriction; it has pains shooting into the left arm, oedema and a quick, throbbing, tense, hard pulse, which may or may not intermit. Carditis and pericarditis may call for Cactus. It presents a better picture of rheumatic carditis than any other remedy. It seems to lie midway between Aconite and Digitalis. It controls the inflammatory condition and strengthens the heart’s contractions, and does not poison the heart like Digitalis or Strophanthus. There is great irritation of the cardiac nerve and Cactus may be found to be the remedy for angina pectoris. It is a remedy adapted to hypertrophy of the heart in young people. It is also very useful in intense palpitation and fluttering sensations about the heart; it is indicated for such symptoms in young girls about the age of puberty and at menstrual epochs. Difficult breathing , suffocative , fainting, violent palpitation and inability to lie down are symptoms indicating the cardiac asthma or dyspnoea.
Kalmia latifolia. [Kalm]
Kalmia is a remedy for cardiac hypertrophy, especially after rheumatism, and has the symptom so common in heart affections, namely , “numbness of the left arm.” There is with Kalmia much pain and anguish about the heart, some dyspnoea, palpitation, and pressure from the epigastrium towards the heart. The heart is irregular and intermits every third or fourth beat. There are shooting pains through the chest to the scapula. Kalmia is an excellent remedy for cardiac troubles when they have been caused by the suppression of rheumatism by external applications. The pulse of Kalmia is slow, but not as slow as Digitalis. Phytolacca has tingling and numbness of the right arm, but the three chief remedies having this symptoms in the left arm are Kalmia, Rhus and Aconite. These pains, as Prof. W.B. Hinsdale points out, should not be considered as “keynotes.” Their symptomatic value consists in pointing to a class of drugs rather than to an individual drug. The minutiae of the pains should be studied. Acute pericarditis depending upon rheumatism will call for Kalmia; the sharp pains taking away the breath will call attention to it. Hering says Kalmia has a most beneficial action in diminishing too rapid pulsation of the heart.
Spigelia. [Spig]
Spigelia is another remedy for the painful affections about the heart. It stands at the head of the list for acute carditis and pericarditis. There are sharp pains shooting from the heart to the back, and radiating from the heart down the arm, over the chest, and down the spine. There is palpitation worse from any movement of the arm or body. There is a purring sensation felt over the cardiac region when placing the hand thereon. The pulse is intermittent, not synchronous with the heart beat, and the slightest motion of the arm or hands makes the patient worse. Heart symptoms accompanying neuralgia call for Spigelia. Irregular and tumultuous action of the heart are well met by Spigelia. At times the heart beat is even audible. We sometimes find this symptom under Arsenicum, which is useful in hypertrophy of the heart from climbing high places, mountains, etc., but Spigelia comes in earlier in heart troubles than does Arsenicum. Rheumatic endocarditis will often find its curative remedy in Spigelia, and it has a most beneficial action in angina pectoris. In cardiac inflammation it comes in after Aconite. It corresponds well to chronic affections of the heart, particularly valvular disease and hypertrophy.
Cimicufuga. [Cimic]
This is a remedy often indicated in heart troubles,especially when they supervene upon chorea or rheumatism of the bellies of the muscles. The headache confined to the forehead or as if the top of the head would fly off is present and an indicating feature. Pain under the left nipple and down the left arm may also be present. The pains is apt to come in shocks. Insomnia is persistent.
Aconite. [Acon]
Among the remedies having a marked influence of the heart is Aconite. It has, as has been seen, numbness of the left arm; it also has tingling in the fingers, associated with heart disease. Aconite produces a cardiac congestion, with anxiety, oppression and palpitation, worse when walking ; lancinating stitches occur, and also attacks of intense pain. It is the remedy in uncomplicated hypertrophy of the heart. In pericarditis and endocarditis when the inflammation sets in with fever with the intense mental anxiety so characteristic of the drug. The 30th acts marvellously in these conditions. Glonoine has a fulness in the region of the heart, with some sharp pains, fluttering of the heart with violent beating,as if the chest would burst open. Labored breathing pains radiating in all directions, even into arms. Must have head high and a pulsating headache to well indicate the remedy. Amyl nitrite has oppressed breathing and constriction about the heart. Both of these latter remedies are useful in angina pectoris. Veratrum viride has a condition simply of intense arterial excitement and is recommended as a remedy to be used continuously in hypertrophy with dilatation. The force and frequency of the pulse are abnormal, as a rule slow, sometimes rapid. It is an important remedy in all inflammatory affections of the heart and its membranes,especially those caused by infections.
Rhus toxicodendron. [Rhus-t]
Rheumatic hypertrophy calls for Rhus. It is a palpitation of the heart from over-exertion, with numbness and lameness of the left arm and shoulder. Pericarditis or endocarditis from exposure to rain, getting wet, etc. These symptoms are worse on every change of the weather. Uncomplicated hypertrophy of the heart such as comes in athletes, machinists, etc., calls for Rhus; and among other remedies for this condition may be mentioned Arnica and Bromine. Pericarditis due to septic condition will call for Rhus, and in heart troubles, as in all others, it follows Bryonia well; and Bryonia may be an early remedy in pericarditis. The rheumatic basis of nearly all the heart symptoms and the general condition of the remedy will decide.
Normocytic Anaemia:
There is a high prevalence of normocytic and normochromic anaemia in COPD patients which is due to erythropoietin resistance at bone marrow level. Low hemoglobin levels are strongly associated with increased functional dyapnoea, decreased exercise capacity and thus affects the functional capacity as well as causes a poorer quality of life. The anaemia is usually resistant to erythropoietin replacement or iron supplementation. Anemia is also an independent risk factor for increased mortality especially in presence of chronic heart failure.
Screening test: Simple hemoglobin and hemogram including RBC morphology should help us diagnose presence of anemia.
Treatment:Whether correction of this anaemia is likely to benefit these patients is uncertain and yet needs to be studied but in a small study, blood transfusion improved the exercise tolerance of patients with anaemia.
Osteoporosis:
The inflammatory mediators of COPD like TNF-α, IL-1β AND IL-6 act as stimulants for osteoclasts which cause bone resorption. In addition COPD patients have several other risk factors for osteoporosis like advanced age, poor mobility, smoking, poor nutrition low BMI and high doses of inhaled corticosteroids as well as courses of oral steroids. Low bone mineral density leads to higher incidence of vertebral compression fractures and peripheral fractures.
Screening Test: X-ray of the hip or vertebrae can be used for screening but the cornerstone for the diagnosis of osteoporosis is a T-score value <-2.5 for total hip scan on dual-energy radiograph absorptiometry (DEXA). In resource limited settings, Bone Mineral Density on Ultrasonography may be used but only as a screening tool and not a diagnostic tool. Serum 25-OH Vit D levels should be done wherever possible.
Prevention of osteoporosis: should be based on the elimination of specific risk factors such as inadequate calcium and vitamin D intake, smoking and sedentary life.
Treatment: All patients with a T-score <-2.5 should be treated for osteoporosis with bisphosphonates and supplements of calcium and Vit D to bring the 25-OH Vit D levels to 30ng/ml (75nmol/L) or higher.
Depression:
Around 40% of COPD cases are affected by severe depressive symptoms or clinical depression due to inactivity, dependence for daily activities as well as for livelyhood, inability to socialize, end of life issues.
Diagnosis: The sixitem Hamilton Depression Subscale appears to be a useful screening tool.
Treatment: Professional help from a psychiatrist if required should be encouraged. Homoeopathic medicines are effective in the treatment of depression in COPD patients, Cognitive-behavioral therapy and psychotherapy provided during pulmonary rehabilitation significantly reduces depression in COPD patients.
Diabetes:
Patients with COPD are at a 50 to 80% higher risk of having concurrent Diabetes even if the COPD is mild. On the contrary, Asthma does not show such an association. The systemic inflammation of COPD, mainly the pro-inflammatory cytokines like TNF-α and IL-6 are believed to induce insulin resistance and increase the risk of type 2 diabetes.
SYSTEMIC MANIFESTATIONS OF COPD
Other Co-morbid conditions: Lung cancers and obstructive sleep apnoea are some other co-morbid conditions which need to be screened for and managed appropriately. As treating physicians, we must have a high index of suspicion for presence of these co-morbid conditions in case of COPD, must screen for these co-morbid conditions and treat them appropriately. Treating the co-morbid conditions not only has a beneficial effect on the COPD but also improves quality of life, reduces morbidity, hospitalizations and the associated financial implications.
Homeopathic Management of COPD Symptoms
Homeopathy is one of the most popular holistic systems of medicine. The selection of remedy is based upon the theory of individualization and symptoms similarity by using holistic approach. This is the only way through which a state of complete health can be regained by removing all the sign and symptoms from which the patient is suffering. The aim of homeopathy is not only to treat COPD symptoms but to address its underlying cause and individual susceptibility. As far as therapeutic medication is concerned, several medicines are available for COPD symptoms treatment that can be selected on the basis of cause, sensation, modalities of the complaints. For individualized remedy selection and treatment, the patient should consult a qualified homeopathic doctor in person. There are some specific homeopathic remedies which are quite helpful in the treatment of COPD symptoms.
Conclusion:
Unlike some diseases, COPD has a clear cause and a clear path of prevention. The majority of cases are directly related to cigarette smoking, and the best way to prevent COPD is to never smoke — or to stop smoking now.
Occupational exposure to chemical fumes and dust is another risk factor for COPD. If you work with this type of lung irritant, talk to your supervisor about the best ways to protect yourself, such as using respiratory protective equipment.COPD is a multidimensional disease which not only affects the lung physiology but also affects the overall health of the individual in terms of significant disability in work, family roles, socialization and functioning in daily life. As the disease progresses, the quality of life gets severely impaired in patients with COPD, and most patients are more bothered by this than their rapid decline in lung function. In routine clinical practice, physiological measures such as lung function test are used to diagnose. It is also important to tackle on timely the co-morbid conditions and requisite homoeopathic medicine should be given to minimize the burden of these co-morbid conditions on the patient.
Posted By
Team Homeopathy 360
You may also like

Thyroid Disorders in Children –...
ABSTRACT – Thyroid disorders in paediatric and adolescent age groups are often missed by...
Miasmatic Approach In Epidemic...
Author:Dr Aparna, BHMS, MD J.S.P.S. Government homoeopathic medical collegeDepartment of...

Life, Science And Homoeopathy [PART-1]
Author: Prof. (Dr.) Goutam Das M. D. (Homoeopathy) [Abstract: This article deals with...

Qualitative Research and Homoeopathic...
INTRODUCTION: In Present era of Medical science like Modern Medicine our Homoeopathic System is...