ABSTRACT
Venous ulcer, the most common and debilitating skin condition of the lower extremity which impairs the general well-being of the individual, causes for VLU include venous hypertension, peripheral arterial occlusive disease, neuropathy secondary to diabetes, vasculitis or a combination of these, older age, obesity, trauma, immobility, congenital absence of veins, deep vein thrombosis (DVT) and phlebitis also are in background. The following case gives an insight of how a homeopathic medicine improves the condition of the patient considering his mental and physical characteristics in venous ulcer condition.
Keywords: venous ulcer, Sulphur, repertorisation.
Abbreviations: deep vein thrombosis (DVT), venous leg ulcers (VLU), International Classification of Diseases (ICD), outpatient department (OPD), thrice a day (TID), fasting blood sugar (FBS), once a day (OD)
INTRODUCTION
Ulcer is a discontinuation in the lining of the skin or mucous membrane which fails to heal.venous ulcer occurs when there is failure of the valves in the veins to stop the blood flow back into the veins, so this backward blood flow causes stasis of the blood resulting in increased pressure in the distal part of lower limb delaying the process of healing, they most often occur at the gaiter area . This venous ulceration accounts for 80 percent of lower extremity ulcerations. The morbidity caused by them has a serious impact on the quality of life(1).
Risk factors for development of venous leg ulcer include older age, female sex, obesity, trauma, immobility, congenital absence of veins, deep vein thrombosis, phlebitis. These ulcers represent the most advanced form of chronic venous disorders like varicose veins and lipodermatosclerosis. its pathophysiology includes venous hypertension,fibrin cuff theory,inflammatory trap theory, dysregulation of various cytokines.(4)
A study published in 2005 estimated the prevalence of chronic wounds in India to be 4.5/1000 population. The incidence of acute wounds was more than double at 10.5/1000 population(2). In a descriptive, cross-sectional study about the clinical profile of venous leg ulcers, it was found that they were frequent in the economically productive age group (36–45 years); with a male preponderance (M: F – 8.4:1)(3).
Its ICD-10-CM diagnosis code is 187.312(6) .Diagnosis includes physical examination, venous ulcers are generally irregular, shallow, and located over bony prominences. Granulation tissue and fibrin are typically present in the ulcer base. Associated findings include lower extremity varicosities, oedema, venous dermatitis, and lipodermatosclerosis. Venous ulcers are usually recurrent, and an open ulcer can persist for weeks to many years. Severe complications include cellulitis, osteomyelitis, and malignant change. Conventional treatment includes oral zinc antibiotics/antiseptics hyperbaric oxygen therapy which have shown no beneficial effect.(5)
CASE STUDY
- Mr.C. aged 52 years, advocate by profession, a resident of Belgavi, Karnataka visited OPD on 8/3/2019 with the complaint of ulcer on the left lower limb(above lateral malleolus) since 1 month onset was gradual, sensation was needle prick in character, the complaint aggravated by touch of air and he was oversensitive to touch of clothes and was better by elevating the leg.
PAST HISTORY
- The patient is a known hypertensive and diabetic since 2005 and was on antihypertensive and hypoglycaemic drugs since then. He also had a history of varicose veins with recurrent venous ulcers on the lower extremity for which he was on compression therapy. His blood sugar levels were very fluctuating with sudden rise in sugar levels and takes 12units TID of insulin therapy.
FAMILY HISTORY
- Patient had a family of diabetes in father, mother and elder sister
PHYSICAL GENERALS
He was a fat and tall person weighing 90 kgs and height 182.88 cms He was dressed in ironed clothes but shirt was torn on the shoulder and cuffs. His appetite was good and regular having desire for curd and sweets. He had increased thirst, with perspiration all over the body. Sleep was disturbed due to severe pain in the lower extremity even by least jerk, he used to have deep sleep between 3-6 am. Thermally, he was a hot patient.
MENTAL GENERALS
During interrogation, he narrated that he could not bear wrong things if anybody committed mistake, then he had to teach them a lesson, Obstinate, did the task completely. He could not bear failure, by hook or crook, the work needs to be done. He wanted to keep himself on no.1 position. He could manage problem solving in difficult situations, he was a planner , an organiser and could lead the team at work .He liked to take risks in life. He wanted surroundings to be clean. He theorised about every subject while talking, he could talk for hours together on one single topic. He said that he didn’t boast himself but kept on praising his work even a small work or help done to others was shown as social service. On observation, it was seen that his shirt was torn but was not bothered and he was just talking about luxuries, riches and extravagance. He said that he was quiet influential and successful in the society, nobody talks anything bad about him.
ON EXAMINATION
On inspection, ulcer was observed on the left lower limb(above lateral malleolus) the border was irregular, oedema was present, there was a blackish appearance of the surrounding skin, slough at the base,the ulcer was measuring 1.5cm in length x1cm in width there was a sticky discharge oozing out of the ulcer which was yellowish in colour..On palpation ,tenderness was present.(fig1)
DIAGNOSIS – Venous ulcer(1).

FIGURE 1:presentation at the time of first visit
ANALYSIS AND EVALUATION OF THE CASE[TABLE 1]
| CHARACTERISTIC MENTALS | CHARACTERISTIC PHYSICAL GENERALS | CHARACTERISTIC PARTICULARS |
| Injustice cannot support Vanity Ambitious Boasting | Desire for curd , Sleep disturbed due to pain Hot patient | Ulcer on left lower limb above lateral malleolus. Needle prick like sensation Worse by touch of the air |
REPERTORIAL TOTALITY [TABLE 2]
| MIND – injustice ,cannot support MIND- vanity MIND – ambition, much ambitious MIND – boaster,braggart SLEEP-disturbed pains by legs EXTREMITY PAIN- ulcerative leg EXTREMITY PAIN- general air open agg. |
MIASMATIC ANALYSIS
Miasmatic analysis was done of the symptoms considered for totality which showed psora-sycosis as the predominant miasm(7)
REPERTORIAL ANALYSIS
Complete repertory was selected for repertorisation and it was done using HOMPATH software(fig2)
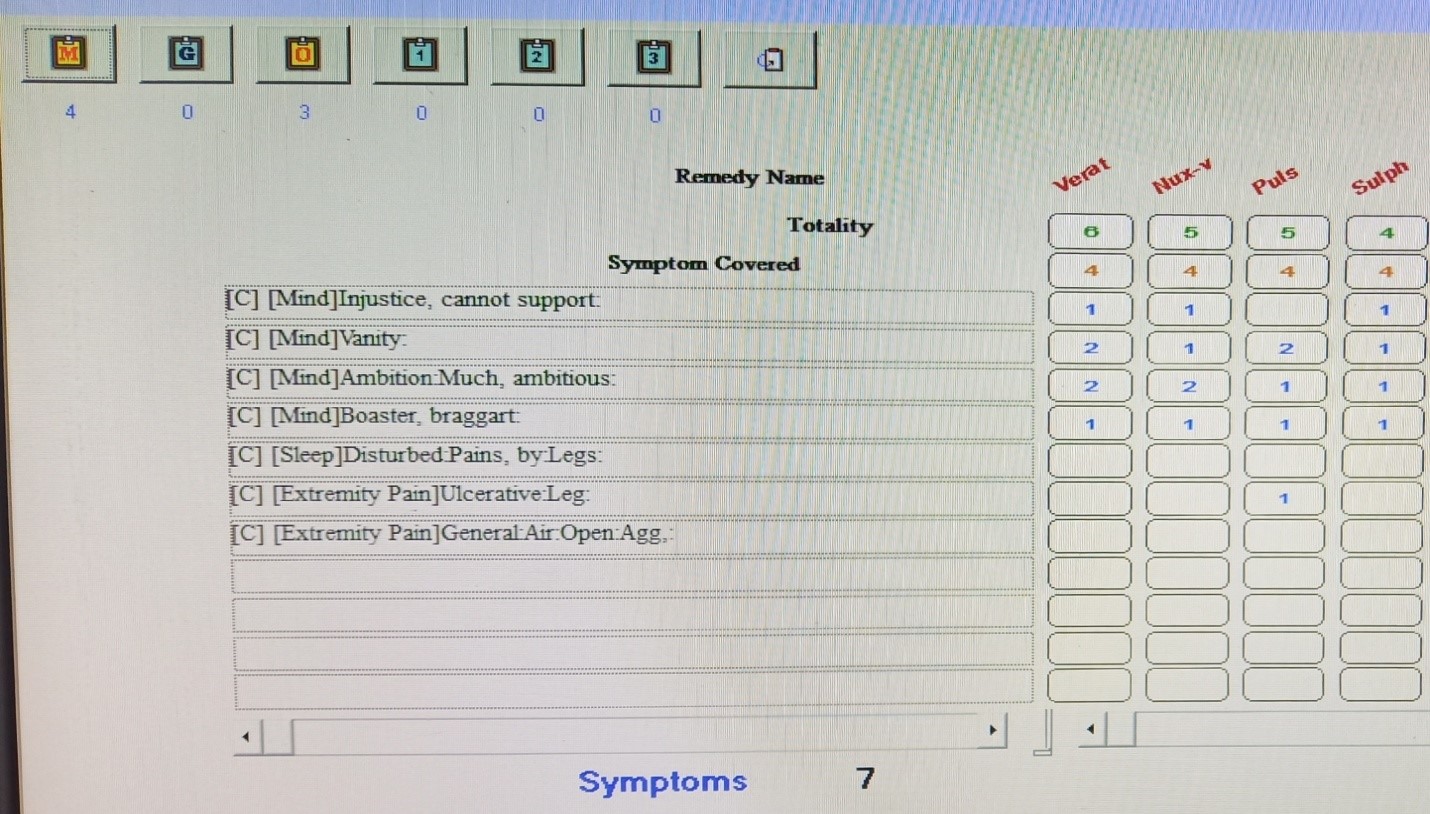
FIGURE 2 : Repertorisation software chart: Hompath classic version 8.0(11)
Repertorial result
Veratrum album – 4/6, Nux vomica, Pulsatilla nigricans – 4/5 , Sulphur – 4/4
THERAPEUTIC INTERVENTION
Patient’s HbA1C – 8% and high FBS He was on insulin therapy 14 units TID with recurrent venous ulcers.
Based on repertorial and miasmatic analysis Sulphur30c OD (powder) for 3 days before breakfast i.e half an hour before followed by placebo twice a day(4 globules) for 15 days was prescribed.
FIRST PRESCRIPTION – 8/3/2019 – Sulphur 30C 3 powders OD and placebo for 15 days
REMEDY JUSTIFICATION
Sulphur was selected as thematic prescription . Patient was a braggrart, with fastidious nature , talked about riches and extravagance but was dressed in rags. Theorised on one single topic for hours together and could build hypothesis on different subjects. He was a hot patient. Depending on the recurrent pathological generals like ulcer on lower extremity and uncontrolled sugar levels, he was advised 30 potency. (12)
FOLLOW UP
The follow ups are shown in table 3 first follow up photograph is shown in (fig3) second follow up
(fig 4). third follow up (fig5)

Figure3 (first follow up),venous ulcer(fig 4) (second follow up) fig 5 (third follow up)
TABLE 3 :FOLLOW UP
| FOLLOW UP DATE | INDICATIONS FOR PRESCRIPTION | MEDICINE WITH DOSES |
| First follow up 25/3/2019 | Pain in lateral malleolus was better Said he did not have pain at all. oedema around the ulcer was reduced by 40 % Sticky discharge reduced by 30 % FBS – 152 mg/dl HbA1C- 6% He did not Take insulin therapy. | placebo was prescribed twice a day for 15 days (4-0-4) |
| Second follow up 10/4/2019 | Initially the patient was oversensitive to touch of air,but at the time of follow up he was experiencing pain only on touch, there was no oozing seen. Ulcer reduced by 70% He has a sound sleep FBS – 130 mg/dl, No insulin | Sulphur 30c 1 Powder OD and placebo- twice aday four pills for 15 days was prescribed (4-0-4) |
| Third follow up 29/4/2019 | On examination – the ulcer was dry, there was no oozing seen ,no edema was present he had a sound sleep. No insulin therapy Case was further observed for 6months till 2020 for any recurrence. | Placebo twice a day for 15 days (4-0-4) No recurrence of Venous ulcer was seen. |
DISCUSSION AND CONCLUSION
Venous ulcer is one of the common and debilitating condition of the current era affecting the quality of life of the affected individual thus impairing his work and also his physical appearance, although they do not cause increased mortality rate but they increase the suffering of the patient from weeks to several years.In conventional treatment the standard care involves the use of compression bandages in venous ulcers On the other hand, antiseptics and antibiotics fail to promote the healing process and to reduce the bacterial density of the wound.(8) A recent Cochrane review confirms this, as there is actually no evidence to support the routine use of systemic antibiotics to promote healing in venous leg ulcers and the available evidence of topical antibiotic and antiseptic efficacy is not strong, and for this reason antiseptic solutions for cleansing the wound are now avoided in routine care of chronic wounds and leg ulcers.(9)
So the case documented here gives an evidence of how homoeopathy can enhance the process of healing in a gentle,rapid and permanent manner as mentioned in aph2(10)and it also improved the general well being of the individual. This case also gives a perception of the improvement and effectiveness of constitutional remedy in venous ulcer condition.
As venous ulcer affects the quality of life and it is one of the debilitating condition, homoeopathy is a boon to the individual affected with this kind of condition reducing its recurrence.
REFERENCES
1)Mishra,S et al(2013). Venous Ulcer: Review Article. Surgical Science. 04.10.4236/ss.2013.42028.
2)Shukla VK,et al. Wound healing research: a perspective from India. International Journal of Lower Extremity Wounds. 2005 Mar;4(1):7-8. doi: 10.1177/1534734604273660. PMID: 15860447.
3)Stephen E, Samuel V. Venous ulcer management: Frontier unconquered. Indian J Vasc Endovasc Surg 2020;7:265-9
4)Vasudevan B. Venous leg ulcers: Pathophysiology and Classification. Indian Dermatol Online J 2014;5:366-70
5)Collins L, Seraj S. Diagnosis and treatment of venous ulcers. Am Fam Physician. 2010 Apr 15;81(8):989-96. PMID: 20387775.
6) ICD-10-CM Codes: L00-L99. 2022 ICD-10-CM Diagnosis Code L97. Available at http://www.icd10data.com
7)Patel RP, Chronic Miasms in Homoeopathy and their cure with classification of their rubrics/symptoms in Dr. Kent’s Repertory , Kerala ,Hahnemann Homoeopathic Pharmacy ,Hahnemann House ,1999.
8)Senet P.phlebolymphology.local treatment of venous leg ulcer.france, paris.pg no.87- 88.2010.vol17available at http://www.phlebolymphology.org
9)O’Meara S,et al. Antibiotics and antiseptics for venous leg ulcers. Cochrane Database Syst Rev. 2010 Jan 20;(1):CD003557. doi: 10.1002/14651858.CD003557.pub3. Update in: Cochrane Database Syst Rev. 2013;12:CD003557. PMID: 20091548.
10) Hahnemann S, Organon of Medicine sixth edition, Delhi, B Jain Publisher Pvt Ltd,1996.
11)Shah J.Hompath classic M.D.Repertory.version 8.0.Mumbai,India:mind technologies.pvt.ltd;2010-2011.
12) Boericke, W.. Boericke’s new manual of homoeopathic materia medica with repertory. New Delhi: B. Jain Publishers. 2007
About Author:
Dr Shweta B. Nanjannavar, MD(HOM)
Prof & Guide, Practice of Medicine
A.M Shaikh Homoeopathic Medical College
And Hospital,Belagavi,Karnataka.
Dr Poojarani.H.Adoni (PG Scholar)
Practice of Medicine
A.M Shaikh Homoeopathic Medical College & Hospital, Belagavi, Karnataka.