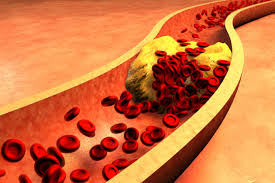
 Hyperlipidemia, or high cholesterol, refers to high levels of fat proteins in the blood.
Hyperlipidemia, or high cholesterol, refers to high levels of fat proteins in the blood.
The condition can affect one fat protein or several. Most people will have no symptoms, but having hyperlipidemia increases the risk of developing heart disease.
| 1. | NAME OF THE CANDIDATE AND ADDRESS (IN BLOCK LETTERS) PERMANENT ADDRESS |
DR SHEENA K N FATHER MULLER HOMOEOPATHIC MEDICALCOLLEGE AND HOSPITAL, UNIVERSITY ROAD, DERALAKATTE, MANGALORE-574160, KARNATAKA. FLAT NO 603, INLAND EXCELLENCY, ARYA SAMAJ ROAD, MANGALORE, KARNATAKA. |
|
| 2. | NAME OF THE INSTITUTION | FATHER MULLER HOMOEOPATHIC MEDICAL COLLEGE AND HOSPITAL, DERALAKATTE, MANGALORE | |
| 3. | COURSE OF THE STUDY & SUBJECT |
M.D.(HOM) ORGANON OF MEDICINE AND HOMOEOPATHIC PHILOSOPHY |
|
| 4. | DATE OF ADMISSION TO THE COURSE | 16 / 6/ 08 | |
| 5. | TITLE OF THE TOPIC : “MIASMATIC EVALUATION OF HYPERLIPIDAEMIA” |
||
| 6. | BRIEF RESUME OF THE INTENDED WORK | ||
| 6.1 NEED FOR THE STUDY: Raised or abnormal levels of lipids & lipoproteins in the blood has become a common clinical problem of the century which has turned out to be a challenge to the physician. It is regarded as a highly modifiable risk factor for cardiovascular disease due to the influence of cholesterol on atherosclerosis. Hyperlipidaemia results from genetic predisposition interacting with an individual diet & lifestyle. More than half the patients with angiographically confirmed premature coronary heart disease have a familial lipoprotein disorder which represents the most common genetic dyslipidaemia with a prevalence of 1 – 2 %. Familial combined hyperlipidaemia characterized by elevated levels of cholesterol or triglyceride or both is estimated to cause 10 – 20 % of premature coronary heart disease & 10 % of myocardial infarction. Secondary hyperlipidaemias constitute the vast majority of cases of hyperlipidaemia met in clinical practice. In type 2 diabetis mellitus 50% cause of death is found to be due to coronary heart disease. Familial cholesterol hyperlipidaemia though being the most common genetic form of hyperlipidaemia, the genetic & metabolic basis of the disorder has hitherto been poorly defined. Early detection & early control of high cholesterol in a person is an important step in reducing the development & progression of coronary heart disease & atherosclerosis. Lowering plasma cholesterol by diet & drugs slows & may even reverse the progression of atherosclerotic lesions & the complications they cause. The expensive mode of treatment & variety of side effects in the other systems of medicine, has created an awareness in the population seeking alternative system of medicine to cure such risk factors at the earlier stage before progression into complications .Homoeopathic system of medicine is safe and based on the individual constitution and totality of expressions. The constitutional method of treatment which includes the miasmatic background of an individual has helped the sick to recover more effectively. A study in this direction is necessary to know the effectiveness of miasmatic treatment in hyperlipidaemia cases Hence this study has been undertaken to define the existence of a relation if any with fundamental & dominant miasm in hyperlipidaemia, so that the evaluation of miasm in an individual can help in early detection of predisposition for hyperlipidaemia & thus help in the prevention. 6.2 REVIEW OF LITERATURE Plasma levels of cholesterol & triglyceride beyond 95th percentile for age & sex is termed hyperlipidaemia. Lipid is an essential chemical in the body. Besides their role in cellular structure, hormones & various other biochemical function, most of the triglycerides are stored in adipose tissue. They are the highly concentrated form of energy which can support body’s energy needs for long periods of food deprivation. Insoluble lipids are solubilized in association with protein as lipoprotein & transported. Chylomicron, Very low density lipoprotein (VLDL), Low density lipoprotein (LDL), High density lipoprotein (HDL) & albumin free fatty acids are different lipoprotein complexes that transport lipid in blood. 50 % is excreted through bile & 50 % is converted to bile acids which are excreted as bile salts. LDL is more atherogenic while VLDL are less atherogenic. HDL helps in removing cholesterol & hence non atherogenic. 1% increase in coronary heart disease risk for each 1% increase in LDL cholesterol & 2 – 3% reduction in coronary heart disease risk for each 1% increase in HDL cholesterol is generally seen Any defect in the synthesis, transport or excretion of the lipids cause a rise in their level in plasma which becomes a risk factor for coronary heart disease which is one of the major cause of death. Etiology Primary causes of hyperlipidaemia
|
|||
| 7. | MATERIALS AND METHODS |
| 7.1. SOURCE OF DATA The subjects of the study will be selected from the patients with hyperlipidemia attending OPD, IPD and peripheral centres of Fr Muller Homoeopathic medical college hospital as per inclusion criteria. 7.2 METHODS OF COLLECTION OF DATA The Materials used for the Study: A minimum of 30 cases would be selected. All these cases would be represented in the standardized case record & analyzed for serum lipids. According to the guidelines given in SCR, case would be analyzed, processed & the miasm erected. Inclusion Criteria:
Exclusion Criteria:
|
| 8. |
LIST OF REFERENCES | |
| 1. Sthyanarayana. U, Chakrapani. U . Biochemistry. 3rd ed. Kolkata : Books & Allied (P) Ltd; 2006. p 285 – 287 2. Vasudevan. D.M, Sreekumari. Text book of biochemistry. 5th ed. New Delhi: Jaypee brothers, Medical publishers (P) Ltd;2007. p 148 – 163 3. Mcphee J. Stephen, Papadakis A. Maxine,Tierney M. Lawrence. 2008 Current Medical Diagnosis and Treatment. 47th ed. USA: Mc Graw Hill; 2008. p1074 – 1076 4. Shah N Siddharth. API Text book of Medicine.7th ed. Mumbai: The Association of physician of India; 2006. p 250 – 257 5. Braunwald, Fauci, Kasper, Hauser, Longo, Jameson. Harrison’s principles of internal medicine Vol II. 15th ed.USA: Mc Graw Hill; 2001. p 2250 6. Hahnemann Samuel. Organon of medicine. 6th ed. New Delhi: B Jain publishers Pvt Ltd; p 94. 7. Vithoulkas George. Homoeopathy medicine for the new millennium.26th ed New york: Arco publishing;2000. p 32,36 8. Dhawale. M.L. Principles and practice of homoeopathy, 3rd ed. Bombay : Institute of clinical research; 2000.p28 9. Dhawale.M.L. Hahnemanian totality symposium Part II Area c.2nd ed. Mumbai: Institute of clinical research; 2000.pc-16,c-19 10. Patel P. Ramanlal. Chronic miasm in homoeopathy and their cure with classification of their rubric/symptoms in Dr.Kent’s repertory, Kottayam: Hahnemann book house;1996. p6, 7,75. 11. www.pubmed.org – hyperlipidemia, September 2008 12. www.wikepedia.com – hyperlipidemia, September 2008 |
||
| 9. | SIGNATURE OF THE CANDIDATE. | |
| 10. | REMARKS OF THE GUIDE. | |
| 11. | 11.1. NAME AND DESIGNATION OF GUIDE (In block letters). |
DR. ROSHAN PINTO, BHMS ,MD (HOM), DEPT. OF ORGANON OF MEDICINE AND HOMOEOPATHIC PHILOSOPHY, FR. MULLER HOMOEOPATHIC MEDICAL COLLEGE, DERALAKATTE, MANGALORE |
| 11.2. SIGNATURE. | |
|
| 11.3. CO-GUIDE. | ||
| 11.4. SIGNATURE. | ||
| 11.5. HEAD OF THE DEPARTMENT. | DR. SHIVAPRASAD K, B.Sc, BHMS MD (HOM), PROFESSOR & HOD, DEPT. OF ORGANON OF MEDICINE AND HOMOEOPATHIC PHILOSOPHY, FR. MULLER HOMOEOPATHIC MEDICAL COLLEGE, DERALAKATTE, MANGALORE |
|
| 11.6. SIGNATURE. | |
|
| 12. | 12.1. REMARKS OF THE CHAIRMAN & PRINCIPAL. |
|
| 12.2. SIGNATURE. |
|
|
Source: www.rguhs.ac.in/cdc/onlinecdc/uploads/06_H002_5559.doc