

Introduction: Irritant contact dermatitis (ICD) is a common inflammatory skin condition which is caused by skin barrier damage from various external and environmental exposures in combination with activation of innate immune responses [1]. ICD is more prevalent than allergic contact dermatitis (ACD), accounting for 80% of all cases of contact dermatitis [2] which can affect both sexes and all ages. The prevalence of contact dermatitis in India is 4.38% [6]. Homoeopathic management of contact dermatitis is safe and cost effective, without the use of topical steroids [3].
Case Summary: A 25-year-old female patient presented with 8-month history of pruritic eczematous lesion on the dorsum of the left foot was successfully treated with individualised homoeopathic medicine, Natrum muriaticum 1M. A detailed case taking, repertorization based on totality of symptoms and thorough reference to materia medica were done to select the similimum. Potency and repetition of dose were modified as per the requirement of the case. There was a significant improvement of the skin lesion without any topical application. This report shows the utility of homoeopathic treatment in contact dermatitis, but further studies are required to assess the effectiveness of homoeopathy in such conditions.
Key words: Irritant contact dermatitis, case report, homoeopathy, individualisation, natrum muriaticum
Introduction: Irritant contact dermatitis is a non-specific inflammatory eczematous skin condition caused by activation of innate immune responses by the pro-inflammatory factors of chemical stimuli. It causes disruption to the integrity of skin with lesions of different degrees of severity [4] according to the concentration, quantity, duration and frequency of exposure of the irritant. It is also based on the characteristics of skin type of the person (dry, oily, thick, thin, tendency of atopy, previously damaged skin) and environmental conditions (temperature, humidity) [5]. Substances which cause irritation in the skin are physical and chemical agents, plants, phototoxic agents, airborne irritants, etc. Physical irritants like abrasions, friction and detergents like sodium lauryl sulfate in combination lead to the condition alone [5]. Symptoms of irritant contact dermatitis include itching, burning, stinging and pain. But pruritus is more common in allergic contact dermatitis. No pathognomonic signs and symptoms are present to differentiate between allergic and irritant contact dermatitis. Its clinical types include acute phase which presents with redness, swelling, oozing, crust formation, vesicles, pustules with tenderness, subacute phase includes crusting, scaling and hyperpigmentation and lichenification can be seen in chronic irritant contact dermatitis [5]. History of signs and symptoms, pattern and distribution of lesions, clinical examination determine the diagnosis of ICD as there is no routine diagnostic test. Patch test can be done to exclude the chance of allergic contact dermatitis [1]. Antihistamines and corticosteroids are used by conventional systems to treat patients with ICD, as there is no specific treatment [6]. Recurrency of the condition and high expenses of medications sometimes prompt patients to find alternative medical systems for treatment. Homoeopathic system of medicine treats the person as a whole, having a holistic approach. Physician collects the symptoms to make a totality which individualises the patient, which lead towards the selection of correct medicine. System treats such conditions based on the principle of individualization without the use of topical steroids.
Patient information
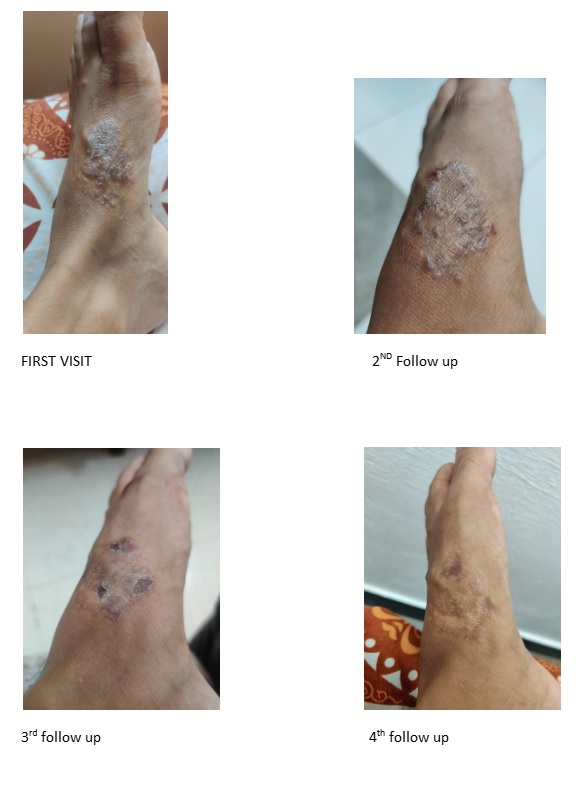
A 25- year- old female patient presented with the complaint of pruritic eczematous eruption in the medial aspect of dorsum of left foot, since 8 months. Itching of the affected area led to scratching which had caused thin, watery discharge from eruptions. Complaint of the patient had started as a vesicle with itching in the medial aspect of the dorsum of left foot, which gradually increased in size. Patient didn’t take any medications for the presented complaint. As the size of the eruption had increased, she decided to take medications.
Past History
Affected area of the skin was burnt ten years back and scar remained. Afterwards patient got similar pruritic eruptions in the same area of the left foot more than two times. She took allopathic medications for the same. Patient had noticed that, such complaints were initiating after wearing new leather chappals, but not all the times. She had chicken pox in the year of 2018.
Family History
Patient’s father had hypertension, ischemic heart disease, renal calculi and mother had dyslipidemia. Paternal grandmother suicided due to depression. No other illnesses in the family were reported.
Personal history
Patient was pursuing her degree and belonged to a middle socioeconomic family.
Clinical findings
Patient was poorly nourished with a mild pallor and oily face. An oval shaped, brownish papulosquamous eruption was present in the medial aspect of the dorsum of the left foot measuring 3.4 cm x 2.5 cm. Her skin was dry and rough.
Generals
Patient had reported that her sleep at night was disturbed due to anxiety related to her studies and family. Thermally the patient could not tolerate the hot climate and heat. She had adequate appetite, but drank only less than 1 L of water per day. Perspiration was normal but offensive. Mentally, he was anxious and sad, but when consoled, felt better. She didn’t talk much.
Diagnostic assessment
The patient was diagnosed with irritant contact dermatitis on the basis of available history and clinical findings.
Therapeutic intervention
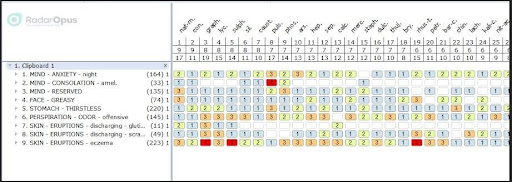
Totality of symptoms of the case was considered and symptoms were repertorised using Kent’s repertory from radar software. Natrum muriaticum had highest score in repertorial analysis. After thorough reference from materia medica, Natrum muriaticum was selected as similimum. 1 dose of Natrum Mur 1M was prescribed at bed time, dissolved in ¼ glass of water, for two weeks.
Follow up and outcomes
Date | Follow up | Prescription |
20-10-23 | Eruption in foot Itching of the eruption Discharge after scratching Disturbed sleep Offensive perspiration |
x 2 weeks |
07-11-23 1st follow up | Eruption in foot- same Itching slightly better Discharge- slightly better Other complaints same |
X 2 weeks |
20-11-23 2nd follow up | Eruption was drying, but no further improvement. Itching- slightly better Discharge- better Disturbed sleep – same Perspiration- offensive |
X 2 weeks
|
06-12-23 3rd follow up | Eruption was drying Itching- better Discharge- better Disturbed sleep- better Offensive perspiration- slightly better |
X 1 week |
17-12-23 4th follow up | Normal skin colour returned (scar of burns was present) No itching, discharge All generals are good Patient feels better mentally. |
X 1 WEEK |
Discussion
Individualised homoeopathic medicine helped to treat the case without any topicals. After detailed case taking, the symptoms were repertorised to get the group of similar remedies from which Natrum Muriaticum was selected as the similimum with the reference of materia medica. Natrum Muriaticum 1M was prescribed based on the totality of symptoms and regular follow-ups were taken. First follow up was satisfactory as itching and discharge were better to the patient. In the second follow up Natrum muriaticum was given in the same potency as eruptions with itching and discharge remained standstill. In third and fourth follow-ups the patient was showing significant improvements. Potency selection and repetition was based on homoeopathic principles. Homoeopathic individualised medicine could treat this case successfully within 2 months.
Conclusion
This case report demonstrates the successful management of irritant contact dermatitis using individualized homeopathic treatment, specifically Natrum muriaticum. A thorough case-taking, repertorization, and materia medica consultation were integral to identifying the similimum. Regular follow-ups and individualized adjustments in potency and repetition ensured a gradual and sustained recovery without the need for topical applications. This case highlights the potential of homeopathic medicine as a safe, effective, and holistic approach for treating skin conditions like ICD, warranting further studies to explore its broader application and efficacy.
Repertorisation
References
- Patel K, Nixon R. Irritant Contact Dermatitis — a Review. Current Dermatology Reports. 2022 Apr 7;11(2).
- Bains SN, Nash P, Fonacier L. Irritant Contact Dermatitis. Clinical Reviews in Allergy & Immunology. 2018 Oct 6;56(1):99–109.
- Signore, DO RobertJ. Classic homoeopathic medicine and the treatment of eczema. www.cosderm.com. cosmetic dermatology; 2011 Sep 24;420-25
- Nosbaum A, Vocanson marc. Allergic and irritant contact dermatitis. Eur J Dermatol. 2009. 19 (4);325-32
- Litchman G, Nair PA, Atwater AR, Gossman WG. Contact dermatitis. PubMed. Treasure Island (FL): StatPearls Publishing; 2023.
- Patel A, Ram H. Irritant contact dermatitis treated with constitutional homoeopathic medicine – A case report. Journal of Integrated Standardized Homoeopathy. 2022 Apr 18;5:24–9.



