HFMD (HAND, FOOT AND MOUTH DISEASE)
Hand, foot, and mouth disease (HFMD or HFM) is a common, self-limiting, viral infection that causes blisters on the hands, feet, and inside or around the mouth. It mainly affects children under the age of 5 years.
HFMD, also called enteroviral vesicular stomatitis, occurs sporadically worldwide. Epidemics are most common during warm weather, usually in the late summer or early autumn.
It is important to note that HFMD is NOT related to foot and mouth disease of animals.
HFMD mostly occurs in children under 10 years of age with 95% of the cases occurring in toddlers aged under 5 years. However, it can also affect older children/adolescents. Adults, especially those who are immunocompromised, may also be affected. However, HFMD only rarely affects healthy adults.

Fig.4. hfmd
Cause:
Enteroviral vesicular stomatitis (HFMD) is usually caused by the Coxsackie virus, most commonly the A16 subtype. It may also be caused by other viruses such as:
Coxsackie A virus (5, 6, 7, 9, 10)
Coxsackie B virus (2, 5)
Enterovirus 71
Echoviruses.
Enterovirus 71 infection is associated with more severe infections that may involve the heart, lungs, and can also cause inflammation of the lining of the brain (meningitis).


Fig. 5. Entero virus

Fig. 6. Life Cycle of Enterovirus
The life cycle of Enterovirus. Enterovirus (EVs) enter the host cells by binding to receptors or by exosome-mediated endocytosis and release positive-strand RNA. The RNA undergoes transcription and translation after being covalently linked to the viral protein VPg (3B). The translated polyprotein is hydrolyzed by various proteases into 10 separate major proteins, including VP0, VP1, VP3, 2A-C, 3A-D, where VP0 is subsequently hydrolyzed to VP2 and VP4. VP1-4 are assigned to participate in the assembly of viral protein coats, while 2A-C, 3A-D are directed to participate in the replication of viral genetic material. Finally, the viral RNA and coat are assembled and processed into mature viruses, which are then co-packaged with host organelle decomposers in vesicles and secreted out of the cell, or directly released by exocytosis
Etiology:
Hand, foot, and mouth disease is a viral exanthem, and it is most commonly caused by the coxsackievirus of the Enterovirus family. Coxsackievirus A16 and enterovirus A71 are the serotypes most commonly implicated as causative agents. Coxsackievirus A6 has recently emerged as another cause of HFMD in the USA and worldwide. Coxsackievirus A10 has been implicated in severe disease. Coxsackievirus A4 to A7, A9, B1 to B3, and B5 have also been less commonly associated with HFMD.
Epidemiology
This viral infection is not indigenous to one area in particular but occurs worldwide. As children (particularly those younger than seven years of age) tend to be infected at a higher rate than adults, you can see outbreaks in daycares, summer camps, or within the family. Large-scale surveillance from China demonstrated that more than 90% of HFMD cases occurred in children less than five years of age, mortality was around 0.03%, and that cases tended to occur more frequently during late spring and early summer. A study from Vietnam showed a positive correlation between an increase in environmental temperature and humidity and an increase in the incidence of HFMD.
In 2021, French surveillance found a rapid increase in HFMD cases, with more than 3400 cases. Although more than 90% of sequenced cases were found to be linked to Enterovirus, atypical cases were found to be associated with Coxsackievirus A6 and A16. Coxsackievirus A6 remains the dominant cause of HFMD in the United States.
Prevelence:
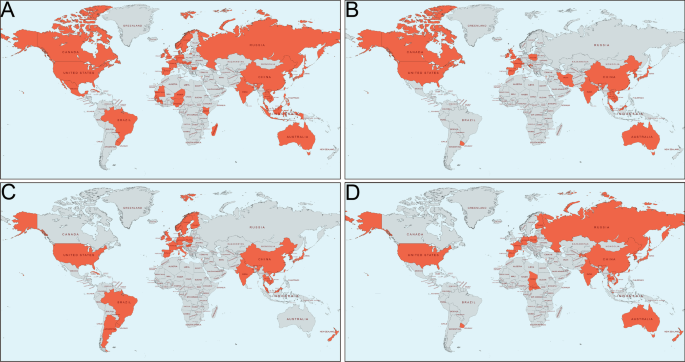
Fig. no 7. Distribution of patients with HFMD in the world. A EV-A71; B CVA16; C CVA6; D CVA10. Areas marked in orange indicate that EV-A71/CVA16/CVA6/CVA10 epidemic have been reported
Pathophysiology:
The spread of the human enterovirus is mediated by oral ingestion of the shed virus from the gastrointestinal or upper respiratory tract of infected hosts or via vesicle fluid or oral secretions.Patients tend to be most infectious in the first week of the disease, with an incubation period ranging between 3 to 6 days.After ingestion, the virus replicates in the lymphoid tissue of the lower intestine and the pharynx and spreads to the regional lymph nodes. This can be spread to multiple organs, including the central nervous system, heart, liver, and skin.

Fig. 8 pathophysiology of hfmd
Transmission:
Transmission occurs via direct contact with blister fluid or droplets spread from the mouth. It can spread very rapidly among family members or within a school. The virus can be shed in faeces and saliva for several weeks.
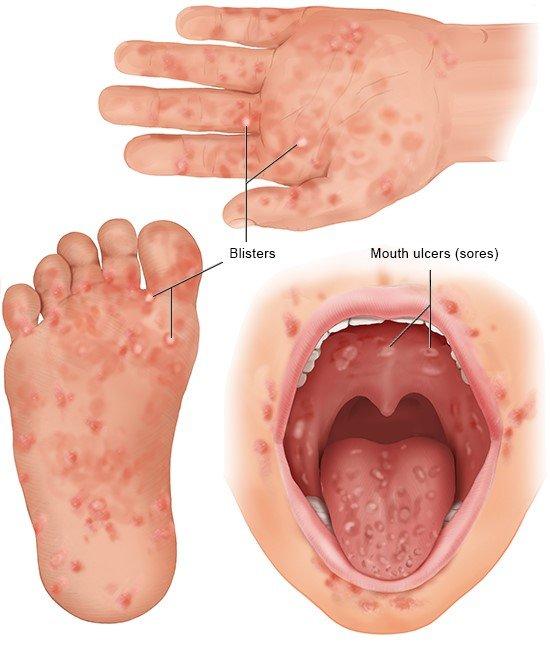
FIG.9 BLISTERS OF HFMD
Clinical features:
The illness usually begins with one or all of the following: fever, sore throat, loss of appetite, and lethargy. However, many children remain well in themselves despite the rash. The blisters usually appear 1—2 days following the fever.
The incubation period is typically 3—6 days and children remain infectious until the blisters have ruptured and healed (usually 7—10 days).
Skin Findings Typically include:
Blisters on the tops of the hands, feet and/or palms, and soles. Lesions usually:
* Feel tender
* Evolve over time from flat pink macules to small, elongated, red-greyish blisters
* Are often oval rather than round
* Peel off within a week, without leaving a scar.
Small blisters (vesicles) and ulcers may develop in and/or around the lips and mouth and the back of the throat. These can sometimes be very painful. Oral intake may be significantly impacted, especially in infants and younger children.
In children with eczema, or past eczema, blisters, flat red macules and papules may develop over other areas of the skin, especially the buttocks and sometimes on the arms, legs, and genital skin.

Fig.10. typical feature of hfmd
Atypical HFMD can result in a more widespread rash and blistering. Features may include:
* Red, crusted macules and papules without blistering
*Large blisters (bulla)
*Targetoid (bulls-eye, or target-shaped) lesions
*Nail shedding
*Involvement of atypical or unusual sites such as the
.

Complication:
Severe complications are very uncommon in people that are otherwise healthy. They include:
* Dehydration due to inadequate fluid intake. This can cause significant problems in younger children.
* Fingernail and toenail changes are often noted about two months after HFMD infections due to coxsackie A6 infection.
Transverse lines in the nail plate that slowly move outwards
Onychomadesis (nail shedding) may occur about 2 months after the illness, however, eventually the nails return to normal.
Serious enteroviral infection can lead to:
Widespread blistering
Enteritis
Myocarditis
Inflammation of the brain and or the lining of the brain (meningoencephalitis)
Loss of nerve function in a limb (acute flaccid paralysis)
Pulmonary oedema and pneumonia
Haemorrhagic conjunctivitis
In pregnancy, viruses that cause HFMD can cause first trimester spontaneous miscarriage or intrauterine growth restriction
Meningoencephalitis, thrombocytopenia, disseminated intravascular coagulopathy, cardiomyopathy and hepatitis in the newborn have rarely been described.
Long-term sequelae of HFMD
Severe HFMD occurs mainly affects preschool children under the age of 5, a crucial stage in their growth and development. Although treatment advancements have led to a decrease in acute mortality, there are still concerns about the potential possible short-term or long-term impacts (Fig. 1).
Neurological Dysfunction
A substantial burden of neurological sequelae following HFMD has been given more attention, especially in severe cases . Among patients who experienced cardiopulmonary failure after CNS involvement, the proportion with subsequent sequelae (facial nerve palsy, limb weakness and atrophy, dysphagia, central hypoventilation, seizure, and psychomotor retardation) was significantly higher compared to those who only CNS involvement. The clinical severity of CNS involvement was significantly related to the childrens neurodevelopment (a delay in the gross motor and personal-social categories, delayed neurodevelopment)Serious virus-associated CNS infection during childhood appear to be associated with the later mental disorders, like attention-deficit hyperactivity disorder (ADHD) diagnosis alongside social/communication/emotion problems and autistic features . Some severe EV-A71 infected patients may experience impaired speech and language skills due to subcortical white matter involvement in the acute stage. Long-term functional neurological morbidity is associated with the involvement of medulla oblongata, gray matter in the brainstem or spinal cord, which may be closely monitored for early intervention and meticulous management
Visual impairment
HFMD-related eye involvement presents variable signs, including pseudomembranous conjunctivitis, outer retinitis and maculopathy , which is only observed in young adult patients in both sexes and always unilaterally. Despite self-limited nature and complete visual recovery in most cases later than resolution of HFMD symptoms (several weeks to months), some cases may have residual visual loss.
Nail abnormalities
Delayed skin and nail change, such as desquamation of palms and soles, Beaus lines, or onychomadesis, have also been observed in some severe EV-A71 infected patients. Nail change, mainly presenting as onychomadesis involving toenails or fingernails, is usually observed among 1—2 months after the onset of HFMD and lasted for 1—8 weeks, most for approximately 4 weeks and the changes are more likely to occur synchronously . It can occur in both children and adults. The pathogens associated with nail abnormalities in HFMD patients are various, but mainly caused by CVA6 . Nail change is usually self-limited with spontaneous healed requiring no treatment for all patients
In addition to focusing on the common health effects of HFMD, other health problems should not be ignored. Allergic diseases: a population-based cohort study has revealed that children suffered from HFMD had decreased risks of asthma . In contrast, another retrospective cohort study found that the risk of asthma was higher in children with herpangina and HFMD . Diabetes: One adult patient with severe atypical HFMD associated with CVA6 viremia showed impaired glucose tolerance after 2-year follow-up . Heart diseases: A population-based cohort study has showed meningitis caused by herpangina/HFMD is the main disease associated with a higher risk of Kawasaki disease . Idiopathic ventricular tachycardia, degenerative aortic valve disease, degenerative mitral valve disease, may be considered as sequelae of CVA6 infection in adults . Nephropathy: A large national cohort study showed that children infected with EVs, particularly coxsackieviruses, had a significantly increased risk of developing nephrotic syndrome . Leukemia: The risk of leukemia was significantly lower in the EVs-infected cohort, and herpangina/HFMD was the main disease reduced the risk of leukemia. Long-term follow-up programs are crucial for early recognition of possible sequelae and early intervention in children who have suffered from HFMD, especially at a young age. Further studies are needed to better understand the pathogenesis of HFMD and its impact on sequelae.

Diagnosis:
HFMD is usually diagnosed clinically. Cutaneous lesions are typically distributed symmetrically over common sites of the skin such as the hands, feet, and in and around the mouth in a child.
Other diagnostic tools include:
Polymerase Chain Reaction (PCR) Testing
Viral DNA may be detected from nasopharyngeal, (throat or nose), swabs and stool specimens.
Analysis of blood, cerebrospinal fluid (CSF), and faeces samples can confirm the diagnosis, but are rarely needed except in atypical or severe cases.

FIG.12 PCR TEST FOR HFMD
Skin Biopsy of a Blister
Very rarely indicated.
Shows acral skin with lymphocytic infiltrates at the epidermis.
The infiltrate is associated with keratinocyte apoptosis in early lesions.
Differential Diagnosis:
Bacterial infections: such as Group A Streptococcus and Staphylococcus aureus, may cause similar blistering skin lesions, eg, bullous impetigo.
Other viral infections such as human parechoviruses, herpes simplex virus, adenoviruses, varicella zoster virus, Epstein-Barr virus, and human herpesvirus 6 and 7.
Bullous insect bite reactions may also present on the hands and feet in children.
Pompholyx eczema.
Differential Diagnosis of Hand-Foot-and-Mouth Disease
Condition
Pathogenesis
Clinical presentation and diagnosis
Treatment
Condition
1. Oral Enanthem
Aphthous ulcer
Pathogenesis
Unknown
C/f
Shallow, round, painful ulcers, measuring
up to 1 cm with surrounding erythema an pseudomembrane
Simple aphthae resolve in one to two weeks, nor
associated with skin lesions.
Complex aphtae tend to be larger occur more frequently, and may indicate systemic disease (eg. gluten sensitive enteropathy) HIV, cyclic neutropenia, systemic lupus erthematous, inflammatory bowel disease, periodic fever , aphthous stomatitis, pharyngitis, or cervical adonis syndrome

Fig.12 oral apthae
Treatment
Simple aphtha supportive care
Complex aphtha treated by underlying cause
Pain relief chlorhexidine Peridex mouthwash lidocaine spray or
ointment, anti inflammatory or corticosteroid
pastes or mouthwash
2. Behcet syndrome
Pathogenesis
Unclear etiology, associated with human leukocyte antigen B51 allele, postulated environmental triggers
C/f
Oral aphthae genital ulcerations, or recurent uveitis
May have arthralgia, vascular or neurologic lesions
Oral lesions are painful round with an erythematous border and are 1 cm to 3 cm in diameter or larger
Fig.13 behcet syndrom
Treatment:
Corticosteroids, azathioprine amuran, cyclophosphamide. Methotrexate, interferon alfa, ustekinumab (stelara)infiliximab (Remicade)etanercept (Entrell)
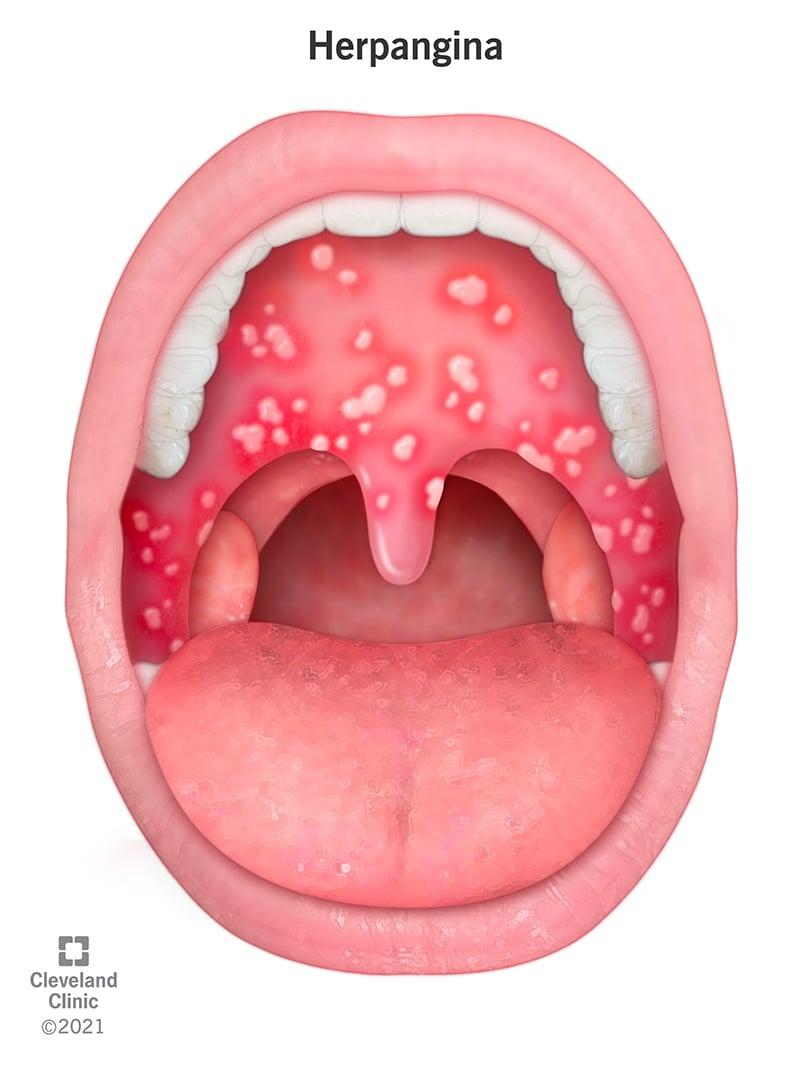
3. Herpangina
Pathogenesis
Соxsakie virua.
Enchovirus
C/f
Oral vesicles that form uncers with associated with inflammation.
Cossackievirus A subtypes 1-6, 8, 10 and 22
Thought to be on a continuum with hand-foot-and- mouth disease
Fig.14 herpangina
Treatment
Supportive care
4.Herpetic gingivostomatotis
Pathogenesis
Неrpes simplex virus 1 and 2
c/f
Fever, and lymphadenopathy, oral erythema and small, oral vesicles on the palate, tongue. gingiva and oral mucosa that form ulcers that may become confluent, vesiclesmay be present on lips
Trunck calls may be present, diagnosis can be made by culture of immunologic assay .

Fig.15herpaetic gingivostomatitis
Treatment
Supportive care acyclovir started in the first 72 hours resulted in faster resolution of oral lesions
5. Pemphigus vulgaris
Caused by desmosome autoantibodies
C/F:
Oral mucosal Bullae and erosions of lips tongue and oropharynx, may affect eyes and genital area, potential life treatning

Fig.16 pemphigus vulgaris
Diagnostic testing with direct immunofluorescence
microscopy or serum testing.
treatment:
Corcoacids, azathioprine, cyclophosphamide, intravenous immunoglobulin.
Maculopapular or vesicular exanthem
Atopic dermatitis:
Genetic, immunologic and environment factors.
C/F:
Erythematous plaques and vesicular lesions, excoriation, dry skin
Younger children with lesions on extensor surfaces, cheeks, older children lesions on flexor surfaces, lesions on hands and feet common.

Fig.17 atopic dermatitis
Treatment:
Avoid triggers (eg cold weather, frequent hot baths, fragrances
detergents)
Emollient cream, topical corticosteroids, oral agents for severe cases.
Bullous Impetigo
Staphylococcus aureus
C/F:
Superficial vesicles pregress to flaccid bullae that rupture, collarette of scales surrounding blister atperiphery of lesion, tends to affect trunk, extremities and moist, intertriginous areas, does not scar, systemic symptoms uncommon.

Fig.18 bullos impetigo
Treatment:
Topical mupirocin (Bactroban) or retapamulin (Altabax) for more extensive disease or inability to tolerate topical therapy may use amoxicillian/ clavulate doxyocyclin
Erythema multiforme:
Immune mediated, often secondary to infection (specificallynherpes simplex virus and mycoplasma pneumoniae) may also be secondary to drugs and other causes.

Fig.19 erythema multiforme
C/F:
Trunk limb, and face distribution, erythema multiforme minor limited to the skin, erythema multiforme major involves mucosal membranes, skin lesions <3 cm in diameter, two concentric colored rings surround dusky central zone, affects 10% of body surface area, often elevated C-reactive protein level
Treatment:
Supportive care if caused by adrug, discontinue that agent, if secondary to herpes simplex virus consider ant- viral therapy, conicosteroids may be used in severe cases although controlled studies are lacking.
Негрes
Caused by herpes simplex virus 1 and 2

Fig.20 herpes simplex
C/F:
Fever, pruritus maculopapular and vesicular rash lesions may appear on areas in contact with oral herpes (eg herpetic whitlow) in areas prone to bodily contact (eg herpes gladiatorum) or on sites of previous atopy (e.g eczema herpeticum)
treatment: acyclovir , famciclovir, or vala cyclovir
Measles:
Caused by measles virus

Fig.21 measles
C/F:
Respiratory spread presents with fever, cough, coryza, Koplik spots (white papules) may present on buccal mucoss before maculopapular that starts on head and spreads distally .Complications include pneumonia, keratoconjunctits, encephalomyelitis
Treatment :
Supportive treatment, vitamin A supplementation measles may be prevented with routine childhood immunization. measles 100,000 per year worldwide.
Rocky mountain spotted fever:
Rickettsia rickettsia transmitted by infected Tick(e g-American dog tick Rocky Mountain wood tick)

Fig.22 rockymountain spotted fever
C/F:
History of a tick bite (50% 60% of pt) headaches, fever, fatigue, nausea, photophobia, rash starts with blanching erythematous macules and papules on wrist and ankles spreads centripetally may ulcerate. Complications include congestive heart failure, dysrhythmia, seizures, nerve palsies.
Treatment:
Doxycycline, preventive measures include avoiding tick infested habitats. tick repellant, full body skin examinations after exposure to areas with ticks
Scabies:

Fig.23 scabies
Linear distribution of papules corresponding with mite burrows, typical distribution includes hands, feet, skinfolds genitalia; intense pruritus, worse at night miles can be visualized in skin scrapings by microscope
treatment:
Permethrin cream 5%(Elimite) wash all clothing, bedding and towels in hot water treat close contacts.
Steven johnson syndrome:
Delayed-type hypersensitivity reaction usually associated with drugs
C/F:
Fever, malaise prodrome, painful skin and mucous membrane (ie, eye, mouth, and genitallia lesions. erythematous with blister formation and carpet lesions pulmonary, renal and hepatic involvement common 10% of sien surface
Discontinue causative drug refer to specialized units leg bum centers may consider comicosteroids novenou imunoglobulin nor cyc
Varicella zoster virus.
Generalized, itchy, vesicular rash female May use acyclor within 24 hours of rash crest, or later a ser cases or in patients who are immunocompromised”, prevent with vaccination avoid asper may consider corticosteroids
may cause pramontis, hepens, encephalith, son rash may become secondarily infected as starte on face and trunk and spreads to rest of body starts wan macules and progres to papules and veu- cles lesions we in all stages at the same time as each other, symptoms last four to seven days
Treatment:
Specific treatment is not usually required for HFMD, and the focus is symptomatic care. HFMD rarely causes serious complications. Antibiotics do not work and should not be given to children with HFMD.
No vaccines or specific antiviral medications are available.
General measures
Pain relief
Simple analgesia such as paracetamol or ibuprofen as needed.
Antiseptic mouthwashes or topical soothing agents (eg, lignocaine) can be used in children with painful oral/palatal ulcers.
Aspirin should not be used routinely due to the risk of Reye syndrome.
Hydration
Constantly offer the child sips of water/juice to prevent dehydration.
If oral intake is poor, nasogastric or intravenous fluids may be indicated.
Blister care
Leave blisters to dry naturally.
Do not pierce/rupture the blisters to reduce contagion.
Keep the blisters clean and apply non-adherent dressings to erosions.
Discomfort because of pain or fever can be treated with weight-based acetaminophen or ibuprofen.7
Oral application of topical lidocaine is not recommended for use in children because of the lack of benefit39 and the potential for harm.40
Antiviral treatments are not available. One clinical trial of acyclovir (n = 13) reported a reduction of fever and skin changes within 24 hours; however, more evidence is needed.41
Evaluation
The diagnosis of hand, foot, and mouth disease is usually made clinically. The virus can be detected in the stool for about six weeks after infection; however, shedding from the oropharynx is generally less than four weeks. Light microscopy of biopsies or scrapings of vesicles will differentiate HFMD from varicella-zoster virus and herpes simplex virus. While serology is not sensitive to making a diagnosis of HFMD, levels of IgG can be used to monitor recovery.
In some centers, serology is used to differentiate enterovirus 71 from coxsackievirus, as this has prognostic significance. Today, polymerase chain reaction assays are available in most centers to confirm the diagnosis of coxsackievirus. A swab of the lesion can detect coxsackievirus or enterovirus using real-time PCR assays
Prognosis
The prognosis for most patients with hand, foot, and mouth disease is excellent. Most patients recover within a few weeks without any residual sequelae. Acute illness usually lasts 10 to 14 days, and the infection rarely recurs or persists. However, some patients with hand, foot, and mouth disease may develop serious complications, which include the following:
Persistent stomatitis is associated with painful ulcers. The pain can be severe enough to limit food intake, and dehydration can result, especially in young children.
Aseptic meningitis can occur, but this is more common with enterovirus 71. This particular virus is associated with a higher rate of neurological involvement compared to coxsackievirus. The individual may develop acute cerebellar ataxia, polio-like syndrome, encephalitis, benign intracranial hypertension, and Guillain-Barre syndrome. The virus is believed to induce damage to the gray matter, resulting in motor dysfunction.
Coxsackievirus can rarely cause interstitial pneumonia, myocarditis, pancreatitis, and pulmonary edema.
Some studies indicate that coxsackievirus infections may also be associated with spontaneous abortions.
Complications
Pneumonia, myocarditis, pancreatitis, and pulmonary edema, as well as serositis involving other major organs, are rarely associated with HFMD. A large meta-analysis of children with HFMD suggested that lethargy, pneumo-edema/pneumorrhagia, seizures, dyspnoea, and coma were risk factors for death in HFMD.The case fatality rate associated with enterovirus 71 was found to be 1.7% in a systematic review and meta-analysis.
Prevention
Handwashing stops the spread of hand-foot-and-mouth disease, specifically after diaper changes and toileting, and before eating.7,42,43
In China, children who “always wash” hands before meals were less likely to contract the disease.8
Disinfect surfaces and fomites (e.g., toys), avoiding close contact and the sharing of personal items such as utensils and cups with infected persons.7,43
Breastfeeding does not impact the incidence of hand-foot-and-mouth disease. Mothers do not need to stop breastfeeding to prevent transmission of disease.8
There are no vaccines or chemoprophylaxis agents available to prevent hand-foot-and-mouth disease and herpangina.7,44
In the United States, exclusion from childcare does not reduce the spread of the disease and is not recommended unless the child is unable to participate or staff are unable to care for the child without compromising the care of other children.45
Vaccine development
Vaccination is considered the most effective and cost-effective approach to control the incidence of HFMD. Currently, there are monovalent and polyvalent vaccines available against the HFMD pathogen. The monovalent vaccines consist mainly of inactivated whole virus vaccines, synthetic peptide and protein vaccines, recombinant subunit vaccines , and recombinant virus-vector vaccine . Currently, the most readily available inactivated whole virus vaccines for EV71 are produced by Sinovac, Vigo, and the Chinese Academy of Medical Sciences (CAMS). Results from a randomised, double-blind phase 3 trial in China showed that the inactivated EV71 vaccine has a 97.4% efficacy rate . The monovalent inactivated virus vaccine candidates for CVA16, CVA10, CVA6, and CVA5 have only been studied in animal models and lack clinical evidence of protection. However, the limited scope of protection offered by monovalent vaccines, which are specific to one genotype, means that they do not provide protection against other EVs-associated cases of HFMD. Therefore, the most effective approach for reducing the incidence of HFMD is to use polyvalent vaccines that have been developed through the combination of effective monovalent vaccines or by constructing chimeric vaccines with different virus serotypes, which can provide better cross-reactivity and protection. Polyvalent vaccines, which aim to improve cross-reactivity, consist mainly of inactivated polyvalent vaccines, polyvalent virus-like particle vaccines, innovative chimeric vaccines, and recombinant virus-vector vaccines. Currently, the inactivated polyvalent vaccines, including bivalent, trivalent, and quadrivalent vaccines, have mainly been tested for their protective effects in animal studies. Vaccines formulated by combining inactivated EV-A71 and CVA16 viruses induced specific immunity against EV-A71 and CVA16 infections in animal models. The CVA6 and CVA10 inactivated whole virus bivalent vaccines have been shown to elicit high levels of neutralizing antibodies in mice . The induction of a strong neutralizing antibody response and cell-mediated immune response was also shown to occur with the administration of inactivated whole virus trivalent vaccines. The antigen-specific and persistent serum antibody responses by quadrivalent vaccines were comparable to those by the respective monovalent vaccines . In addition, polyvalent virus-like particles, novel chimeric vaccines, and recombinant virus-vector vaccines have all shown to induce broad protective effects and enhance systemic immune responses . Antigenic peptide-based vaccine development and DNA/RNA vaccine technology be also applied for future exploration of polyvalent vaccines. However, it is important to carefully consider the inclusion of appropriate strains and to thoroughly evaluate the immunogenicity and immune interactions when developing multivalent vaccines.
THERAPEUTICS
BELLADONNA :-
Belladonna acts upon every part of the nervous system, producing active congestion, furious excitement, perverted special senses, twitching, convulsions and pain. Belladonna always is associated with hot, red skin, flushed face, glaring eyes, throbbing carotids, excited mental state, hyperæsthesia of all senses, delirium, restless sleep, convulsive movements, dryness of mouth and throat with aversion to water, neuralgic pains that come and go suddenly. Heat, redness, throbbing and burning. Great childrens remedy. Scarlet fever. Exophthalmic Goitre. Corresponds to the symptoms of “air-sickness” in aviators. Stands for violence of attack and suddenness of onset.
MOUTH:- Dry. Throbbing pain in teeth. Gumboil. Tongue red on edges. Strawberry tongue. Grinding of teeth. Stammering. Foul odor from mouth. Mouth feels hot. Dry, burning mouth, with great thirst. Paralytic weakness of internal parts of mouth. Mouth feels scalded. Dryness of whole inner lining of cheek, tongue, which looks as if burnt, roof. Slimy mouth in morning, when awaking, with pressing headache. Thick, white mucus collects in mouth and throat, with constant inclination to hawk and swallow. Saliva thickened, tenacious, brownish, white, clings to tongue like glue. Salivation ; < when lying down. Salivation succeeding dryness of mouth. Increased flow of saliva.
THROAT:- Troublesome continued dryness of mouth, lips and throat with a violent longing for drink, but not satisfied by it. Dryness of mouth and pharynx, with sense of constriction of throat. Tonsillitis ; < right side ; parts bright red ; < swallowing liquids. Sore throat : fauces and pharynx deep red ; soft palate and tonsils swollen ; swallowing painful, particularly fluids ; speech thick ; feels like a lump in throat, which induces hawking ; throat swollen outside and sensitive to touch.
FEVER:- Feels very chilly, wants warmth of a stove. Angina. Cool hands forehead, with much thirst, but no fever.Chill in evening, mostly on arms, with heat of head. At noon : coldness, with marbled skin and blue lips. Several attacks of fever in one day, during which hot stage followed cold within a few minutes to half an hour after, always without thirst in either stage, and mostly with confusion of head. Heat of forehead, with cold cheeks. Internal chill, with external burning heat. Coldness of limbs, with heat of head. During hot stage : delirium ; redness and puffiness of face, great thirst. Inflammatory, catarrhal, rheumatic, milk, puerperal and typhoid fevers, with furious delirium and loss of consciousness. Temperature of skin very much raised ; skin scarlet. Sweat : on covered parts ; with or immediately after heat.
SKIN:- Painful sensitiveness of skin to contact. Heat over whole body, with bluish redness of whole surface. Skin imparts a burning sensation to examining hand. Heat, redness and dryness of skin. Red, hot swelling of affected parts. Skin scarlet, smooth and shining. Erythema of skin. Urticaria. Resembling mosquito-bites ; itches most mornings and evenings ; scratching feels pleasant. Phlegmonous erysipelas ; bright red and radiating. Vesicular erysipelas. Eruptions like roseola and scarlet fever, with fever, sore throat, cough, headache, etc.
MERC SOL:-
A human “thermometer”. Indicated in the secondary stage of syphilis where there is a febrile chloro-anaemia. Tremors everywhere. Symptoms are worse at night, from warmth of bed, from damp, cold, rainy weather, worse during perspiration.
MOUTH:- Sweetish metallic taste. Salivary secretions greatly increased; bloody and viscid. Saliva fetid, coppery. Speech difficult on account of trembling tongue. Gums spongy, recede, bleed easily. Sore pain on touch and from chewing. Whole mouth moist. Crown of teeth decay. Furrow in upper surface of tongue lengthwise. Tongue heavy, thick; moist coating; yellow, flabby, teeth-intended, feels as if burnt, with ulcers, Fetid odor from mouth, can smell it all over room. Alveolar abscess, worse at night. Great thirst, with moist mouth. Aphthae of children, stomacace. Pain, swelling and ulceration of salivary glands. Bluish color of inner cheeks. Scurvy.
THROAT:- Throat constantly dry ; it hurt as if too tight posteriorly ; a pressure in it if he swallowed, yet he was constantly obliged to swallow, because mouth was always full of water. Suppuration of tonsils, with sharp, sticking pain in fauces when swallowing. Erysipelatous inflammation of throat. Syphilitic ulcers in throat and mouth.
FEVER:- Generally gastric or bilious, with profuse nightly perspiration; debility, slow and lingering. Heat and shuddering alternately. Yellow perspiration. Profuse perspiration without relief. Creeping chilliness. Alternate flashes of heat in single parts. Sweat : profuse, offensive ; does not >, may even < suffering. Complaints increase during sweat. Intermittent fever. Continued or remittent fevers. Worm fever, with intestinal inflammation and diarrhœa. Hectic fever, especially of children. Mucous fever, with prostration. Catarrhal, rheumatic fever, after catching cold.
Typhoid fevers. Yellow fever.
SKIN:- Yellow skin. Yellow fever. Icterus. Jaundice, with biting itching over abdomen. Skin chafed, sore. Itching over whole body, especially at night in bed, when getting warm. Itching that becomes pleasant on scratching. Erythema, upon which vesicles form and pour out a thin, clear fluid. Round spots shining through skin, of a coppery red color. Itch : dry, rash-like, easily bleeding ; fat, especially in bends of elbows, some of vesicles become pustular. Skin dirty yellow, rough and dry ; scaly, dry tetters ; eruptions of not inflamed, little red elevations, points of which peel off.
RHUS TOX:-
The effects on the skin, rheumatic pains, mucous membrane affections, and a typhoid type of fever. Tearing asunder pains. Septicaemia.
MOUTH:- Tongue red and cracked; coated, except red triangular space at the tip; dry and red at edges. Corners of mouth ulcerated; fever-blisters around mouth and chin. Pain in maxillary joint. Sleeps with open mouth. Breath : putrid, excessively so in typhoid fever and diphtheria. Mouth dry, with much thirst. Saliva bloody ; runs out of mouth during sleep. Much tough mucus in mouth and throat.
THROAT:- Sore, with swollen glands. Sticking pain on swallowing. Parotitis; left side. Sensation of dryness in throat. Great thirst and dryness in throat, in typhoid conditions. Sore throat as from an internal swelling, with bruised pain, also when talking, with pressure and stinging when swallowing.
Throat sore, feels stiff ; after straining throat.
FEVER:- Chilliness : in house, toward evening, creeping coldness all over ; and heat in evening, face seemed very hot, though cheeks were cold to touch, and pale, breath hot ; in back and head, heat on anterior part of body ; as if cold water were poured over him, or as if blood were running cold through veins. Cough during chill ; dry, teasing, fatiguing. Great restlessness during chill. During chill, pains in limbs, and during fever twitchings. Chill increased by drinking. Heat : with great thirst ; after the chill, with sweat which relieves. During fever, nettlerash ; thirst, drinking little and often. During sweat : sleep ; urticaria passes off with violent itching. Night sweat, with miliary itching eruption. Suppressed foot sweat.
SKIN:- Red, swollen; itching intense. Vesicles, herpes; urticaria; pemphigus; erysipelas; vesicular suppurative forms. Glands swollen. Cellulitis. Burning eczematous eruptions with tendency to scale formation. Eczema : surface raw, excoriated ; thick crusts, oozing and offensive ; if face is attacked there is œdema of loose cellular tissue about eyelids ; burning, itching, tingling pains ; incessant itching and scratching ; the more they scratch the greater the urgency to scratch. Urticaria from getting wet ; during rheumatism ; with chills and fever ; < in cold air. Carbuncles, bluish, gangrenous. Hardness of skin with thickening. Warts : especially on hands and fingers ; large, jagged, often pedunculated, exuding moisture and bleeding readily.
BORAX:-
Gastro-intestinal irritation. Salivation, nausea, vomiting, colic, diarrhoea, collapse, albuminuria, casts and vesical spasm. Delirium, visual changes, haematuria, and skin eruptions have all been observed from over-dosing. Dread of downward motion in nearly all complaints. Frequently been verified, especially in the therapeutics of children. Of much value in epilepsy. Aphthous ulceration of mucous membranes.
MOUTH:- Aphthae. White fungous like growth. Mouth hot and tender; ulcers bleed on touch and eating. Painful gumboil. Taste of “cellar mould”. Salivation with difficult dentition.
FEVER:- Chill and chilliness mostly during sleep. Chill predominating, especially in afternoon and evening. Chill and heat alternating. Chill from uncovering. Chill passing downward. Thirst not constant ; is generally wanting during chill. Flushes of heat, morning and evening. Hot head, mouth and palms, of infant. Heat or sweat, with inclination to uncover. Sweat during the morning sleep.
SKIN:- Sensation as if a cobweb were lying upon skin of face or hands. Severe itching on back of finger joints ; must scratch them violently.
Red papulous eruption on cheeks and around chin. Herpetic eruption on nates. Skin pale or livid. Wilted, wrinkled skin. Children with aphthae. Ulcerated places on feet from rubbing of shoe or boot.
PHYTOLACCA:-
Aching, soreness, restlessness, prostration. Pre-eminently a glandular remedy. Glandular swellings with heat and inflammation. Decrease of weight. Retarded dentition.
MOUTH:- Teething children with irresistible desire to bite the teeth together. Tongue red tip, feels rough and scalded; bleeding from mouth; blisters on side. Mapped, indented, fissured, with yellow patch down center. Much stringy saliva. Profuse saliva, sometimes yellowish, often thick, ropy, tenacious ; mercurial ptyalism, with inflamed gums.
Salivation with metallic taste in mouth. Diphtheria. Ulcerated sore mouth.
THROAT:- Dark red or bluish red. Throat feels rough, narrow, hot. Tonsils swollen, especially right; dark-red appearance. Shooting pain into ears on swallowing. Cannot swallow anything hot. Ulcerated sore throat and diphtheria; throat feels very hot; pain at root of tongue extending to ear. Uvula large, dropsical. Quinsy; tonsils and fauces swollen, with burning pain; cannot swallow even water. Mumps. Follicular pharyngitis.
FEVER:- Coldness, faintness, dyspnoea ; limbs cold, head and face hot. Chill : every morning ; sudden, followed by fever after confinement ; at night without special fever. Heat : with pain in joints ; high fever. Sweat : cold on forehead ; toes sweat ; night sweat, having an acid reaction. High fever, alternating with chilliness and great prostration.
SKIN:- Disposition to boils. Venereal buboes. Skin cool, shrivelled, dry, lead-colored. Barbers itch. Tinea capitis ; shingles. Ringworm ; herpes circinatus. Squamous eruptions, pityriasis ; psoriasis. Lichen-like eruptions, with great itching of skin. Lipoma. Scarlet eruption all over body. Scarlatina ; high fever, headache, both sides of throat covered with membrane, with rash on body. Red spots. Syphilis.
GRAPHITES:-
This remedy is an anti-psoric of great power, but especially active in patients who are rather stout, of fair complexion, with tendency to skin affections and constipation, fat, chilly, and costive, with delayed menstrual history, take cold easily. Particular tendency to develop the skin phase of internal disorders. Eradicates tendency to erysipelas.
MOUTH:- Rotten odor from mouth. Acid, foul odor from mouth. Breath smells like urine. Burning blisters on tongue, salivation. Saliva runs from mouth in morning on stooping. Dryness of mouth in morning.
THROAT:- Palate and fauces somewhat reddened. Violent catarrh in fauces, with sensation as though food had to pass over a lump in throat ; roughness and rawness in throat. Ulcerative pain in throat.
Roughness and rawness in throat.
FEVER:- Chilliness in morning, in bed. Chill and chilliness, most in evening. Chill in evening, with headache and tearing in limbs, great thirst and profuse perspiration after midnight, lasting till morning. Child < after meals, > after drinking, > in open air. Sometimes feet are icy-cold, again quite burning. Flushes of heat. Hands and soles of feet hot and burning. Sweats from slightest motion. Sweat on front of body and centre of chest. Sweat stains yellow, is sour and offensive smelling, and frequently cold. Fetid sweat. Profuse sweat on feet ; they swell and become sore. Profuse night-sweat. Entire inability to sweat. Glands are affected, along with hectic ; discharge gluey ; chills and fever.
SKIN:- Itching over various parts of body, very violent, even on face and genitals. Great itching, as though foreign matter would pass through skin. Continual itching, < at night. Nightly heat. Keratitis. Prurigo in children, with sore, raw places on skin. Skin dry, inclined to crack. Excoriation of skin, especially in children. Raw, moist places between fingers and on face. Unhealthy skin ; every injury suppurates. Skin is not inclined to heal, ulcerates readily. Cracks or fissures of ends of fingers and nipples, labial commissures, of anus, between toes, etc. Herpes exuding a sticky matter.
NATRUM MURIATICUM:-
The prolonged taking of excessive salt causes profound nutritive changes to take place in the system, and there arise not only the symptoms of salt retention as evidenced by dropsies and oedemas, but also an alteration in the blood causing a condition of anaemia and leucocytosis. A great remedy for certain forms of intermittent fever, anaemia, chlorosis, many disturbances of the alimentary tract and skin. Great weakness and weariness. Oversensitive to all sorts of influences.
MOUTH:- Scorbutic gums. Numbness, tingling of tongue. Vesicles and burning on tongue, as if there was a hair on it. Eruptions around mouth and vesicles like pearls on lips. Tongue mapped. Aphthae on tongue, gums and cheeks, with great burning and impeded speech. Saliva : profuse, watery ; salty ; bloody ; constant spitting. Salivation : with thrush, mumps or toothache ; after use of mercury ; in smallpox ; obstinate. Ranula ; chronic inflammation of salivary glands.
THROAT:- Throat feels very dry, yet constantly hawks transparent mucus. Hawking of salty tasting mucus. Sensation of splinter sticking in throat. Feeling as of a plug in throat, with chronic sore throat. Follicular inflammation of pharynx ; after swabbing with nitrate of silver.
FEVER:- Constant chilliness and want of animal heat. Frequent internal chilliness. Chill predominates, mostly internal ; hands and feet cold. Chilliness over whole body, with heat in forehead, pressure in region of root of nose and violent thirst. Chilliness, with frequent yawning. Fever : with violent headache. Rheumatic fever, with chilliness. Hay fever, with watery discharges from eyes and nose. Typhus fever when stupor and chilliness are great ; twitchings.
SKIN:- Crawling sensation all over body, beginning at feet and gradually ascending. Great rawness and soreness of skin ; smarting ; intertrigo. Vesicles, with watery contents, burst and leave a thin scurf. Herpes : about mouth and on arms and thighs ; humid on scrotum and thighs ; during fevers ; in bends of elbows and knees ; moist oozing. Nettlerash : over whole body ; large red blotches, with violent itching ; after violent exercise ; chronic urticaria. Miliary eruption all over. Eczema, raw and inflamed. Smallpox, with salivary flow, confluence of pustules and drowsiness. Boils, small ; blood-boils. Warts in palms of hands. Corns. Scars become painful and redden. Effects of insect bites ; stings of bees, mosquitoes.
HEPAR SULPH:-
Suits especially scrofulous and lymphatic constitutions who are inclined to have eruptions and glandular swellings. Unhealthy skin. Blondes with sluggish character and weak muscles. Great sensitiveness to all impressions. Sweating patient pulling blanket around him. The tendency to suppuration is most marked. The lesions spread by the formation of small papules around the side of the old lesion. Chilliness, hypersensitiveness, splinter-like pains, craving for sour and strong things are very characteristic. Feeling as if wind were blowing on some part. Pellagra.
MOUTH:- Offensive odor from mouth, as from disordered stomach, which he himself notices. White aphthous pustules on inside of lips and cheeks and on tongue. Ulcers on gums and in mouth, base resembling lard.
THROAT:- When swallowing, sensation as if a plug and of a splinter in throat. Quinsy, with impending suppuration. Sore throat ; tonsils so much swollen as to leave no opening visible. Tonsils enlarged, red ; throat and pharynx raw, and studded over with enlarged reddish follicles. Stitches in throat, extending to ear, < when swallowing food.
FEVER:- Sensitiveness to open air, with chilliness and frequent nausea. Great chilliness in open air ; must get to warm stove ; heat feels agreeable but does not relieve. Desire to be covered even in a warm room. Internal chill, with weariness and soreness in all the limbs. Nettlerash, with violent itching and stinging, disappears as heat begins. Dry heat of body at night, with sweaty hands, which cannot tolerate being uncovered. Dry burning heat, with redness of face and violent thirst, all night. Sweats easily, by every, even slight motion. Cold, clammy, frequently sour, offensive smelling sweat. Hectic fever with intermittent paroxysms.
SKIN:- Yellowness of the skin. Constant offensive exhalations from body. Child smells sour. Great sensitiveness of skin to touch and to slightest cold. Unhealthy, suppurating skin ; even slight injuries maturate ; every cut or hurt suppurates. Cracking of skin and smarting of hands and feet. Burning itching on body, with white vesicles, after scratching. Itching rash in bend of knees and elbows. Eczema, spreading by means of new pimples appearing just beyond the old parts. Humid soreness on genitals. Herpes zoster, from spine around left side to median line ; vesicles, bullae, some containing dark pus ; acute neuralgic pains in seat of eruption. Chronic urticaria, eruption chiefly in hands and fingers. Miliary rash in circles. Bleeding of an ulcer, even on slight wiping. Mercurial ulcers.
Bryonia alba
Acts on all serous membranes and the viscera they contain. Aching in every muscle. The general character of the pain here produced is a stitching, tearing; worse by motion, better rest. These characteristic stitching pains, greatly aggravated by any motion, are found everywhere, but especially in the chest; worse pressure. Mucous membranes are all dry. The Bryonia patient is irritable; has vertigo from raising the head, pressive headache; dry, parched lips, mouth; excessive thirst, bitter taste, sensitive epigastrium, and feeling of a stone in the stomach; stools
large, dry, hard; dry cough; rheumatic pains and swellings; dropsical effusions into synovial and serous membranes.
Bryonia affects especially the constitution of a robust, firm fiber and dark complexion, with tendency to leanness and irritability. It prefers the right side, the evening, and open air, warm weather after cold days, to manifest its action most markedly.
Children dislike to be carried or raised. Physical weakness, all-pervading apathy. Complaints apt
to develop slowly.
Mind
Exceedingly irritable; everything puts him out of humor. Delirium; wants to go home; talks of business.
Mouth
Lips parched, dry, cracked. Dryness of mouth, tongue, and throat, with excessive thirst. Tongue coated yellowish, dark brown; heavily white in gastric derangement. Bitter taste (Nux; Col). Burning in lower lip in old smokers. Lip swollen, dry, black, and cracked.
Respiratory
Soreness in larynx and trachea. Hoarseness; worse in open air. Dry, hacking cough from irritation in upper trachea. Cough, dry, at night; must sit up; worse after eating or drinking, with vomiting, with stitches in chest, and expectoration of rust-colored sputa. Frequent desire to take a long breath; must expand lungs. Difficult, quick respiration; worse every movement;caused by stitches in chest. Cough, with feeling as if chest would fly to pieces; presses his head on sternum; must support chest. Croupous and pleuro-pneumonia. Expectoration brick shade, tough, and falls like lumps of jelly. Tough mucus in trachea, loosened only with much hawking. Coming into warm room excites cough (Nat carb). Heaviness beneath the sternum extending towards the right shoulder. Cough worse by going into warm room. Stitches in cardiac region. Angina pectoris (use tincture).
Skin
Yellow; pale, swollen, dropsical; hot and painful. Seborrhoea. Hair very greasy.
Fever
Pulse full, hard, tense, and quick. Chill with external coldness, dry cough, stitches. Internal heat. Sour sweat after slight exertion. Easy, profuse perspiration. Rheumatic and typhoid marked by gastro-hepatic complications.
Modalities
Worse, warmth, any motion, morning, eating, hot weather, exertion, touch. Cannot sit up; gets
faint and sick. Better, lying on painful side, pressure, rest, cold things.
CHAMOMILLA
German Chamomile
The chief guiding symptoms belong to the mental and emotion group, which lead to this remedy in many forms of disease. Especially of frequent employment in diseases of children, where peevishness, restlessness, and colic give the needful indications. A disposition that is mild, calm and gentle; sluggish and constipated bowels contra-indicate chamomilla. Chamomilla is sensitive, irritable, thirsty, hot, and numb. Oversensitiveness from abuse of coffee and narcotics. Pains unendurable, associated with numbness. Night-sweats.
Mind
Whining restlessness. Child wants many things which he refuses again. Piteous moaning because he cannot have what he wants. Child can only be quieted when carried about and petted constantly. Impatient, intolerant of being spoken to or interrupted; extremely sensitive to every
pain; always complaining. Spiteful, snappish. Complaints from anger and vexation. Mental calmness contraindicates Chamom.
Face
One cheek red and hot; the other pale and cold. Stitches in jaw extending to inner ear and teeth. Teeth ache worse after warm drink; worse, coffee, at night. Drives to distraction. Jerking of tongue and facial muscles. Distress of teething children (Calc phos; Terebinth).
Throat
Parotid and submaxillary glands swollen. Constriction and pain as from a plug.
Respiratory
Hoarseness, hawking, rawness of larynx. Irritable, dry, tickling cough; suffocative tightness ofchest, with bitter expectoration in daytime. Rattling of mucus in child’s chest.
Skin
Miliary eruption, with itching and nocturnal tickling.─Unhealthy skin; every injury tends to ulceration.─In the ulcers, tingling, itching, burning, and jerking shootings, with excessive sensibility to the touch.─Itching pimples form around the ulcer, covered with scurf, and suppurating.
Yellow colour of the skin (over the whole body).─Rash of infants and during nursing.─Red rash on the cheeks, on the forehead.─Inflammatory swelling of the glands.
Modalities
Worse, by heat, anger, open air, wind, night. Better, from being carried, warm wet weather
SULPHUR
Sublimated Sulphur
This is great Hahnemannian anti-psoric. Its action is centrifugal-from within outward-having an elective affinity for the skin, where it produces heat and burning, with itching; made worse by heat of bed. Inertia and relaxation of fiber; hence feebleness of tone characterizes its symptoms. Ebullitions of heat, dislike of water, dry and hard hair and skin, red orifices, sinking feeling at stomach about 11 am, and cat-nap sleep; always indicate Sulphur homeopathically. Standing is the worst position for sulphur patients, it is always uncomfortable. Dirty, filthy people, prone to skin affections. Aversion to being washed. When carefully-selected
remedies fail to act, especially in acute diseases, it frequently arouses the reactionary powers of the organism. Complaints that relapse. General offensive character of discharge and exhalations. Very red lips and face, flushing easily. Often great use in beginning the treatment of
chronic cases and in finishing acute ones.
Mind
Very forgetful. Difficult thinking. Delusions; thinks rags beautiful things-that he is immensely wealthy. Busy all the time. Childish peevishness in grown people. Irritable. Affections vitiated; very selfish, no regard for others. Religious melancholy. Averse to business; loafs-too
lazy to arouse himself. Imagining giving wrong things to people, causing their death. Sulphur subjects are nearly always irritable, depressed, thin and weak, even with good appetite.
Mouth
Lips dry, bright red, burning. Bitter taste in morning. Jerks through teeth. Swelling of gums; throbbing pain. Tongue white, with red tip and borders.
Throat
Pressure as from a lump, as from splinter, as of a hair. Burning, redness and dryness. Ball seems to rise and close pharynx.
Respiratory
Oppression and burning sensation in chest. Difficult respiration; wants windows open. Aphonia.Heat, throughout chest. Red, brown spots all over chest. Loose cough; worse talking, morning, greenish, purulent, sweetish expectoration. Much rattling of mucus. Chest feels heavy; stitches, with heart feeling too large and palpitating pleuritic exudations. Use Tinctura sulphuris. Stitching pains shooting through to the back, worse lying on back or breathing deeply. Flushes of heat in
chest rising to head. Oppression, as of a load on chest. Dyspnoea in middle of night, relieved by sitting up. Pulse more rapid in morning than in evening.
Fever
Frequent flashes of heat. Violent ebullitions of heat throughout entire body. Dry skin and great thirst. Night sweat, on nape and occiput. Perspiration of single parts. Disgusting sweats.Remittent type.
Skin
Dry, scaly, unhealthy; every little injury suppurates. Freckles. Itching, burning; worse scratching and washing. Pimply eruption, pustules, rhagades, hang-nails. Excoriation, especially in folds (Lyc). Feeling of a band around bones. Skin affections after local medication. Pruritus, especially from warmth, is evening, often recurs in spring-time, in damp weather.
Modalities
Worse, at rest, when standing, warmth in bed, washing, bathing, in morning, 11 am, night, from
alcoholic stimulants, periodically. Better, dry, warm weather, lying on right side, from drawing up
affected limbs.
1. Arsenic alb 30 : It is effective at the initial stage Dose : 4 times / 1 day
2. Mercsol 200 : For curative BID / 2 days, Prophylactic BID / 1 day
3. Rhustox 30 : When there is stiffness and lameness. It follows Merc. sol Dose : 4 times / 2-3 days
4. Nat. Mur 30 : When there is debility and weakness and can be given after 2 weeks. It follows Rhustox Dose : Q.I.D. / day
5. Fer. Phos 6x + Kali mur 6x : When there is pyrexia and respiratory signs, Repeated every 3 hrs at initial stage
6. Borax : When weakness, debility and inflammation Dose : Q.I.D
7. Five phos 6x + Alfaalfa 6 + Ipeca 30 : for speedy recovery and panters Dose : BID for 7 to 10 days
Reportorial approach:
Kent repertory:
FACE CHAPTER:
Face, eruption, vesicles
vesicles : Aeth., agar., alum., am-c., am-m., anac., ant-c., ant-t., ars., benz-ac., bor., calc-s., canth., carb-an., carb-s., caust., cic., cist., clem., Crot-t., dulc., eupho., ferr-i., graph., hep., indg., kali-ar., kali-bi., kali-i., kali-n., lach., mag-c., Manc., mang., merc., mez., nat-a., nat-c., Nat-m., nat-s., nit-ac., ol-an., petr., ph-ac., phos., plb., Psor., ran-b., Rhus-t., rhus-v.,samb., Sep., sil., stram., stront., sulph., syph., valer., zinc.
acrid : Caust., rhus-t.
ERUPTIONS, vesicles, burning
burning : Agar., anac., aur., caust., cic., nat-m., ran-b.
cold air : Dulc.
confluent : Crot-t., ran-b., rhus-t., sulph.
itching : Anac., ant-c., ars., cic., mez., sep.
varioloid, like : Ant-c.
white : Clem., hell., sulph., valer.
yellow : Agar., ant-c., ars., cic., com., crot-t., dulc., eupho., kreos., manc., merc., nat-c., ph-ac., Rhus-t., rhus-v., sep.
chin, on : Agar., anac., canth., cic., crot-t., hep., manc., nat-c., Nat-m., nat-s., nit-ac., sanic., sars.
forehead : Am-c., arn., bor., canth., kali-i., mez., nat-m., plb., psor., rhus-v., stront.
lips : Agar., ail., alum., am-m., ant-t., asc-t., aur., berb., bor., bov., calc-s., carb-an., chel., chin-s., cic., clem., com., con., hell., hep., kali-p., kali-s., lac-c., lact-ac., mag-c., mag-m., mang., merc., nat-c., Nat-m., nat-s., nit-ac., par., plat., rhod., sang., sanic., seneg., sil., valer.
lower : Agar., ail., aur., com., mag-m., nat-s., par.
upper : Agar., alum., am-m., cic., kali-p., mag-p., mang., rat., rhus-v., seneg., valer., zinc.
blood blisters : Nat-m.
mouth, around : Bor., hell., Nat-m., nat-s.
corners : Agar., caust., cic., mez., seneg., senn.
nose : Am-c., clem., crot-t., lach., lact-ac., mag-c., mag-m., mez., nat-c., nat-m., nit-ac., petr., phel., phos., plb., Rhus-t., sil., verat.
centre, on : Carb-ac.
inside, right : Carb-an., lach., phos.
root : Nat-m.
septum : Am-c., crot-h., thuj.
tip : Nit-ac.
wings : Chel., Nat-m., sil., thuj.
right : Nat-c.
MOUTH CHAPTER:
APHTHÆ: Acet-ac., aeth., agar., all-s., alum., anan., apis., arg-m., ars-i., Ars., arum-t., asim.,aur-m., aur-s., aur., Bapt., berb., Bor., brom., bry., calc., canth.,
caps., carb-ac., carb-an., carb-s., carb-v., caul., cean., cham., chin-a., chin.,
chlor., cic., clem., cocc., corn., cub., dig., dulc., ferr., gamb., hell., hep., hippoz.,
hydr., iod., jug-c., kali-ar., kali-bi., kali-br., kali-c., Kali-chl., kali-i., kali-s., kreos., lac-c.,lac-d., lach., lact-ac., lyc., mag-c., Merc-c., Merc., Mur-ac., myric., nat-a., nat-c., nat-h., nat-m., nit-ac., nux-m., Nux-v., ox-ac., phos., phyt., plan., plb., ran-s., sal-ac., sanic., sars., sec., sil., staph., Sul-ac., Sulph., ter., thuj., vinc.
Mouth , apthae, children, in : Bor., casc., kali-chl., Merc., mur-ac., nux-m., nux-v., plan., sacc., Sul-ac., sulph.
Skin chapter
Skin eruption,
burning : Anthr., apis., ars., coloc., crot-c., crot-h.,
SKIN
ERUPTIONS, rash, scarlet
scarlet : Acon., Am-c., ars., Bell., Bry., calc., carb-v., caust., chlol., coff., com., dulc., hyos., iod., ip., kali-bi., lach., merc., ph-ac., phos., rhus-t., sulph., zinc.
scratching, after : Am-c., am-m., ant-c., bov., bry., calc., carb-s., caust., dulc., graph.,
ip., lach., led., merc., mez., ph-ac., phos., puls., rhus-t., sars., sel., sil., spong., staph., sulph., verat., viol-t., zinc.
slow evolution of rash in eruptive fevers : Bry.
stinging, biting : Nat-m., viol-t.
red : Acon., agar., Am-c., anac., anan., ant-c., apis., arn., ars., aur., berb., calc., cham., chel.,chin-s., chlol., cic., clem., cocc., com., con., cop., crot-t., cycl., dulc., fl-ac., graph., kali-bi., Kali-c., kali-s., lach., lyc., mag-c., Merc., mez., nit-ac., ox-ac., petr., ph-ac., Phos., rhus-t., sabad., sars., sep., sil., spig., staph., stram., Sul-ac., Sulph., thuj., til., valer., vip.
EXTREMITIES CHAPTER:
Extremities ,eruption , hand
vesicles : Anac., arg-n., brom., calc., canth., cic., graph., indg., kali-chl., kali-s., mez., phos.,psor., Rhus-t., rhus-v., sol-n., Sulph., zinc.
burning : Mez.
Extremities, eruption, foot
Foot : Anan., ars., aster., bar-c., bov., calc., carb-o., caust., chin-s., con., croc., crot-c., elaps., genist.,lach., med., mez., phos., rhus-t., rhus-v., sec., sep., stram., sulph.
FEVER CHAPTER:
EXANTHEMATIC fevers, measles : Acon., am-c., ant-c., Apis., ars., Bry.,
camph., carb-v., cham., chel., chin., chlor., coff., cop., crot-h., dros., Euphr., gels., hep., hyos., ign.,
ip., kali-bi., phos., Puls., rhus-t., squil., stram., Sulph., verat., zinc.
scarlatina : Ail., Am-c., Apis., arg-n., arn., ars., arum-t., Bell., bry., calc., canth., carb-ac., carb-v., c
ham., chin., crot-c., crot-h., cupr., Echi., gels., hep., hyos., ip., Lach., Lyc., Merc., mur-ac., Nit-ac.,
nux-m., ph-ac., phos., Rhus-t., sec., stram., sulph., Ter., zinc.