
Abstract: This article presents a chronic case of Tinea Manuum, i.e., fungal infection that occurred over the dorsum of both hands which was distressing to the patient during his day-to-day activities. He had initially taken Steroid ointment for local application but got temporary relief only, leading to recurrence. After a thorough evaluation at our hospital, he was prescribed appropriate homoeopathic remedies selected using totality of symptoms and Kent’s Repertory. He responded very well to the selected remedies and the lesions visibly improved over the course of treatment.
The case study demonstrates that Homoeopathic management in such chronic cases of Tinea Manuum and other similar fungal infections can lead to significant improvement of symptoms and overall patient satisfaction.
Keywords: Case Report, Constitutional Medicine, Tinea, Sulphur, Natrum Muriaticum, Tinea Manuum
Introduction:
“Mycoses” or Fungal infections causing disease in the human body are very common in the tropical and sub-tropical regions of the world including India. The mycosis caused by fungi specifically over Skin, Hair and Nails is called Dermatophytosis, Tinea or Ringworm and the causative agents are termed Dermatophytes. The term “Tinea” is derived from the Latin word for worm and the term “Ringworm” describes the clinical appearance of typical skin lesion, which is annular, resulting from progressive central clearing. These dermatophytes are keratinophilic, and hence they grow in the keratin of the Stratum Corneum layer of the Epidermis.
Sources of infection:
- Soil (Geophilic)
- Animals (Zoophilic)
- Human (Anthropophilic)
3 genera of Dermatophytes commonly implicated are:
- Trichophyton (affect skin, hair & nails)
- Microsporum (affect skin & hair)
- Epidermophyton (affect skin & nails)
Trichophyton rubrum is by far the most common dermatophyte responsible for Tinea.
Risk factors:
- Heat and humidity of tropical climate
- Poor nutrition and hygiene
- Contact with infected animals, infected people or fomites
- HIV infection, Diabetes Mellitus, or any autoimmune disease
Clinically, fungal infection due to dermatophytes can be classified as follows:
- Depending upon the site of involvement,
- Scalp – Tinea capitis
- Face – Tinea faciei
- Beard area – Tinea barbae
- Groins and Buttocks – Tinea cruris
- Hands – Tinea manuum
- Feet – Tinea pedis
- Body – Tinea corporis
- Nails – Tinea unguinum
- Steroid-modified tinea: Tinea incognito
- Due to hypersensitivity to dermatophyte: Dermatophytids
Tinea Manuum is a superficial dermatophyte infection affecting the dorsum of hands, palm and interdigital spaces, having features of itching, and well-demarcated, sharply circumscribed, erythematous, annular lesions with raised leading edges, central clearing with shiny silvery-white scaling on the periphery. It can present both unilaterally and bilaterally. Diagnosis is mostly through clinical observation and relevant history.
Homoeopathic management of such cases of Tinea involves analysis of the local and general symptoms and their modalities taking into consideration the intensity, peculiarity, stage and duration of the disease.
.
Case study:
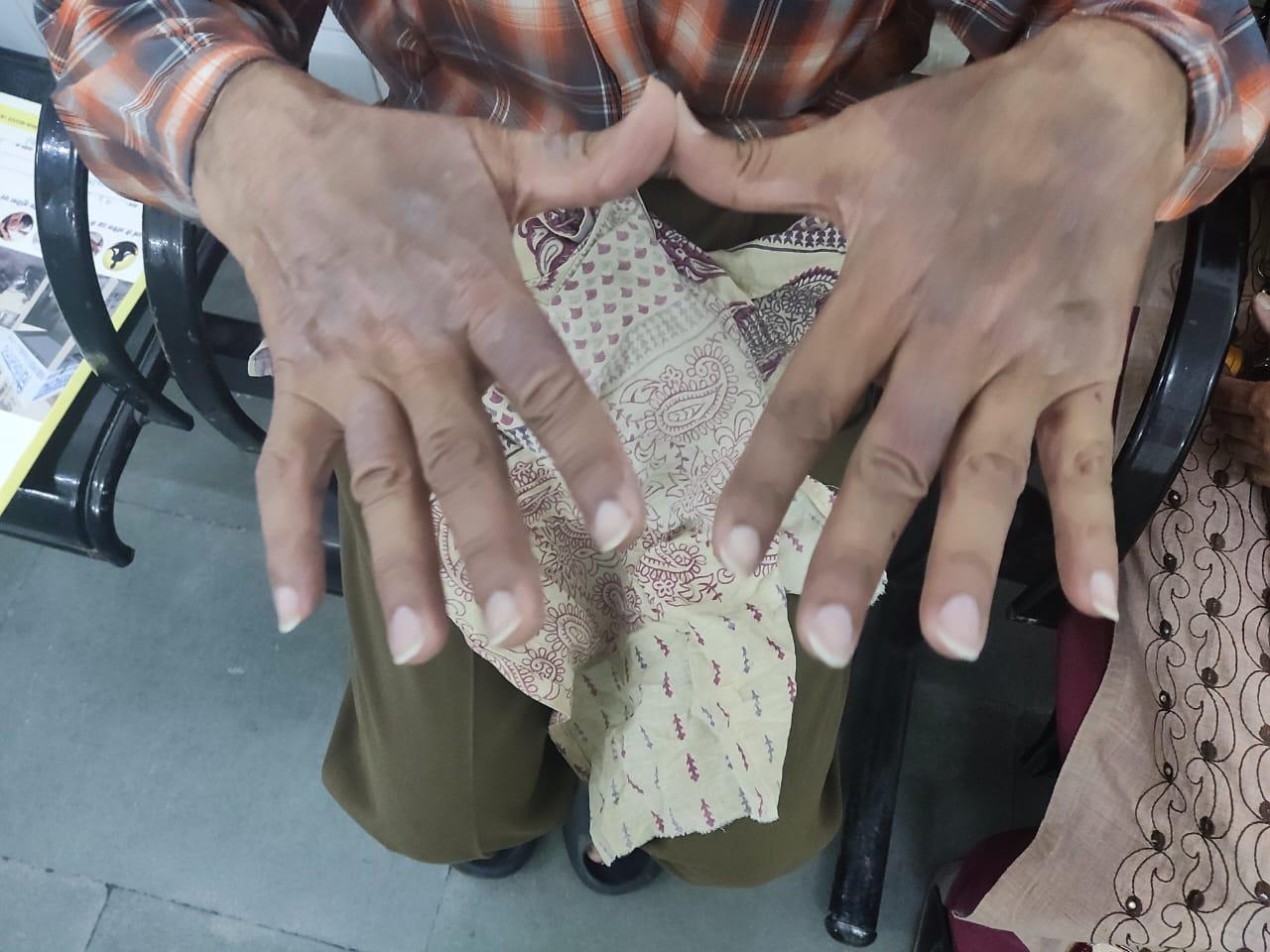
A 64 years old Male patient presented himself to our OPD with multiple erythematous patches over the dorsum of both hands and wrist, associated with intense itching since last 1 year. The symptoms got aggravated with exposure to sunlight and during periods of stress, while local application of Moisturisers ameliorated them. He was initially treated with Steroid ointments which provided temporary relief only. Gradually the lesions flared up again and did not respond to further conventional treatment.
The person did not suffer from any significant medical conditions or drug addictions. No relevant family medical history was found.
In general, the patient is thinly built and has oily skin. He craves oily food, is sensitive to heat and likes cool ambience. He is an introvert by nature, prefers to stay alone and has consolation aggravation. He is recently aggrieved by the sudden loss of his business and remarks that after that incident only the lesions have come up.
Totality of symptoms:
- Itching with red eruption on both hand
- < Sun Exposure, > by moisturiser
- Ailments from business loss
- Hot patient
- Desires salty things
- Alone desire
- Consolation <
- Introvert
- Grief due to business loss
- Thin built, oily skin
Miasmatic analysis:
Miasmatic analysis of all the presenting symptoms were processed with the help of comparison of the chronic miasms, which shows mixed miasmatic condition with the predominance of Psora.
Repertorisation:
Proper case taking was done as per the directions of the homoeopathic principles. After analysis and evaluation of the symptoms of the case, the totality was constructed and the case was repertorised with help of Kent’s repertory in Zomeo Elite software and a group of relevant drugs are found. The repertorial chart is shown in Figure 1.
1st Prescription:
08/02/23 Rx. Sulphur 30/ stat dose (Clinical picture shown in Figure 2)
(At the start of Treatment, Sulphur was given as patient had been using Steroid ointment for a long time)
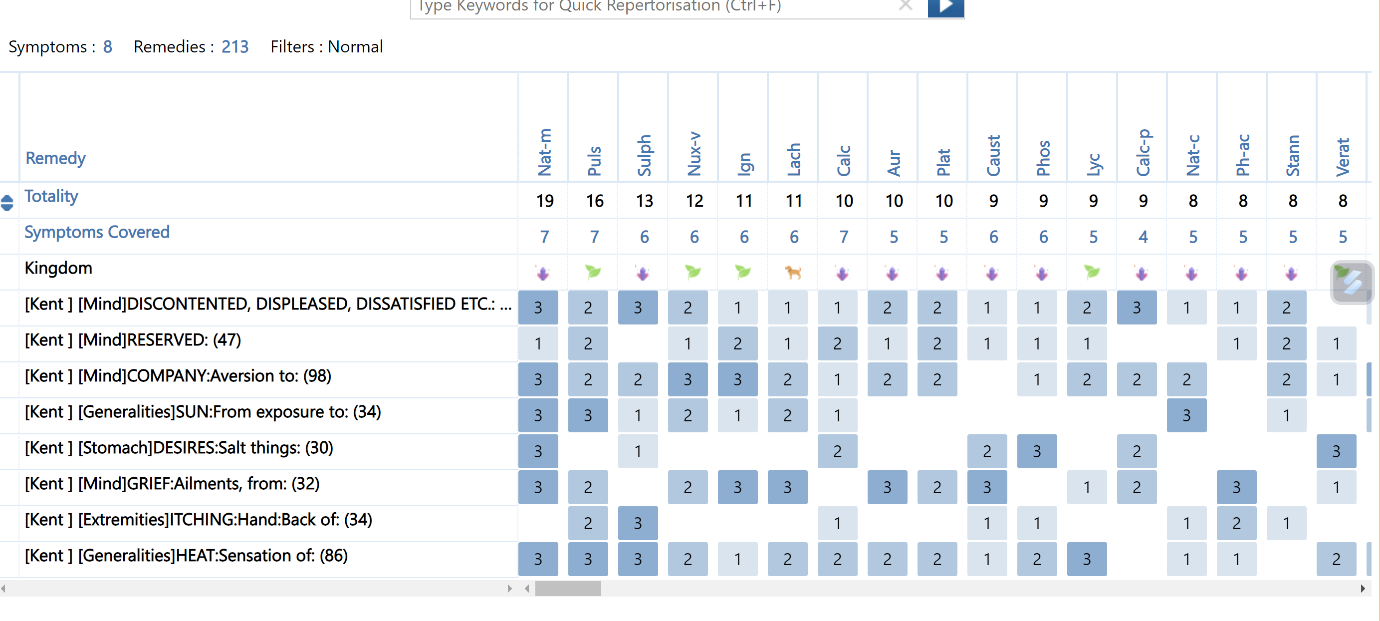
Figure 1: Repertorisation using Kent’s Repertory
Follow up Visit details:
| Dates | Symptoms | Prescribed medicine | Reference Images |
| 18/03/23(2nd Visit) | Severe itching and redness, some eruption upon fingers | Belladonna 30 / OD (for temporary reduction in redness) | Figure 3 |
| 08/04/23(3rd Visit) | Slight decrease in redness, rest of the symptoms remain unchanged | 1.Natrum Muriaticum 30 / OD x 7days2.Echinacea Q / LA with coconut oil | Figure 4 |
| 25/04/23(4th Visit) | 10% decrease in redness, slight decrease in itching | 1.Saccharum Lactis 30 / OD x 10days2.Echinacea Q / LA | — |
| 09/05/23(5th Visit) | 50% decrease in all symptoms | Same medicines to continue | Figure 5 |
| 20/05/23(6th Visit) | 80% improvement in all symptoms | Saccharum Lactis 30 / OD x 10days | Figure 6 |
| 24/06/23(7th Visit) | A small round eruption over right Hand | Natrum Muriaticum 30 x one dose | Figure 7 |
| 10/07/23(8th Visit) | No symptomsSkin is clear | No medicine required | Figure 8 |
Clinical Images:

( Figure 2: First Day of Visit on 08/02/2023 – Sulphur was prescribed )

( Figure 3: 2nd Visit on 18/03/2023 – Severe Itching & Redness after Sulphur administration )

( Figure 4: 3rd Visit on 08/04/2023 – Minimal Reduction, Nat. Mur. Started )

( Figure 5: 5th Visit on 09/05/2023 – Noticeable Improvement in both Redness and Itching )
( Figure 6: 6th Visit on 20/05/2023 – Further Improvement )

( Figure 7: 7th Visit on 24/06/2023 – Small round eruption over Right Hand )

( Figure 8: 8th Visit on 10/07/2023 – Complete Resolution of Skin Lesion, No Symptoms )
Conclusion:
The presented case report showcases the successful treatment of Tinea Manuum and restoration of the wellbeing of the patient with the help of constitutional homoeopathic medicines, further stressing upon the need for Repertorisation in individualised homoeopathic prescription. However, this is a single case study and further well-designed clinical studies may be required to establish homoeopathy as one of the reliable treatment modalities available to patients in the therapeutic landscape of Tinea Manuum.
Declaration of Consent:
The author certifies that she has verbally explained to the patient all details regarding the study and obtained all relevant clinical information in the appropriate patient form, including his informed consent to participate in the study and for sharing of Images and other clinical information.
Conflicts of Interest:
The author declares no conflict of interest.
References:
- Thappa DM. Textbook of Dermatology, Leprology & Venereology, 4th Ed. London: Elsevier Health Sciences APAC; 2013.
- Davidson’s Principles and Practice of Medicine, International Edition, 24th Ed.: Elsevier Health Sciences; 2022.
- Kent JT. Repertory of the Homeopathic Materia Medica. New Delhi: B. Jain; 2016.
- Boericke W. Boericke’s New Manual of Homoeopathic Materia Medica with Repertory, 3rd Ed.: New Delhi: B. Jain Publishers; 2007.
- Rajamohanan R, Raj R, Chellam J, Rengasamy M. Epidemiological Trends and Clinicomycological Profile of Chronic Dermatophytosis: A Descriptive Study from South India. Indian J Dermatol 2021; 66:445
- Verma S, Madhu R. The Great Indian Epidemic of Superficial Dermatophytosis: An Appraisal. Indian J Dermatol 2017; 62:227-36
- Mufeeda CP, Mohan U, Jain P. Effectiveness of Homoeopathic treatment in case of Tinea Corporis and Tinea Cruris: A Constitutional Approach. International Journal of Homoeopathic Sciences. 2022;6(3):29-35.
- Murgod SM. Tinea Corporis and Homoeopathic Management. Int J Hom Sci. 2021;5(4):123
- Laskar B, Paul S, Chattopadhyay A, Karuppusamy A, Balamurugan D, Bhakta P, Das S, Pal S, Singh NK, Koley M, Saha S. Individualized Homeopathic medicines in the Treatment of Tinea Corporis: A Double-blind, Randomized, Placebo-controlled Trial. Homeopathy. 2022 Sep 19;112(02):074-84.
- Murgod, S. M., & Shah, K. (2022). A Systematic Review on Efficacy of Homoeopathic medicines in Tinea infections (Ringworm). International Journal of Health Sciences, 6(S3), 4631–4636. https://doi.org/10.53730/ijhs.v6nS3.6948



