Abstract
Epidermoid Cysts are a sub-type of keratinized cysts which can form in any part of the body but are most commonly found in the areas of neck, back, behind the ear, scalp, etc. They contain a white cheesy material in them and are often wrongly referred to as Sebaceous Cysts, as they do not actually arise from sebaceous glands nor do they contain sebum. The chances of recurrence of epidermoid cysts are high if not drained completely and the lining of the cysts is removed. This article presents a case of elderly female who developed an epidermoid cyst on her back and it was successfully treated non-invasively with Homoeopathy only and a follow up of almost 2 years to highlight that there has been no recurrence since then.
Introduction
Cysts are pathological sac-like structures that contain liquid, semi-solid or gaseous matter in them. They can occur in any part of the body. Histologically the cysts occurring in the skin can be classified into 2 broad categories – Keratinous cysts and Sebaceous cysts. [1][2]
The Keratinous cysts can be of further of two – Epidermoid and Trichilemmal.[1]
In Epidermoid cysts the lining of the cyst is like the normal epidermis whereas that in cases of trichilemmal cysts resembles the external root sheath.
As epidermoid cysts are lined by epidermis and produce stratum corneum and are often surrounded by a tough, fibrous capsule. When the contents of the cyst find their way into the dermis, considerable inflammation results. A foul-smelling, semi-solid material is formed due to degeneration of the contents of the cyst. This semi-solid material resembles sebum and therefore these cysts are mistakenly termed as sebaceous cysts. Steatocystoma multiplex are true forms of sebaceous cysts.[1][2]
Common Site
Epidermoid Cysts
– Face, neck, upper back, post auricular region. Trichilemmal Cysts – Most commonly
found on scalp
Morphology of Epidermoid Cysts[1][2]
- Small to medium sized cysts
- Either skin coloured or yellow
- Usually freely mobile over underlying structures
- Adhered to the skin
- Have a central punctum through which cheesy material can be expressed
Complications[1]
- Secondary infection
- Can induce foreign body reaction if ruptures on the dermis
- Can undergo Dystrophic calcification
Case
A female patient aged 58 years came to the clinic with a complaint of painful swelling on dorsal back region. She has a history of recurrent epidermoid cyst on the same site treated with incision and drainage. The swelling grows gradually becomes inflamed and later on discharges yellow pus. On examination it was found to be hard in consistency, non-mobile, painful to touch.
Physical Generals: Thermal reaction – hot patient. Her appetite is normal. Thirst: 2-3 lit/day. She had desires for sweets, ice cream. Stool and urine was normal. She has tendency to sweat profusely on head and back in hot weather.
Local and systemic examination: The mass was cystic in consistency, non-mobile, painful on touch. Her vital parameters were all within normal limit.
Analysis of the case:
Classification – Dynamic Chronic True Maismatic Surgical Local Disease[3]
As the case presented is a one sided local disease with lack of any characteristic mental symptoms, the physical particular and general symptoms are given more importance in repertorization.
Totality
Desire – sweets Desire – Ice-creams
Perspiration – profuse on back Perspiration – profuse on head Discharges – Thick yellow
Skin – Cysts
Repertory Used – Complete
Repertory[5]
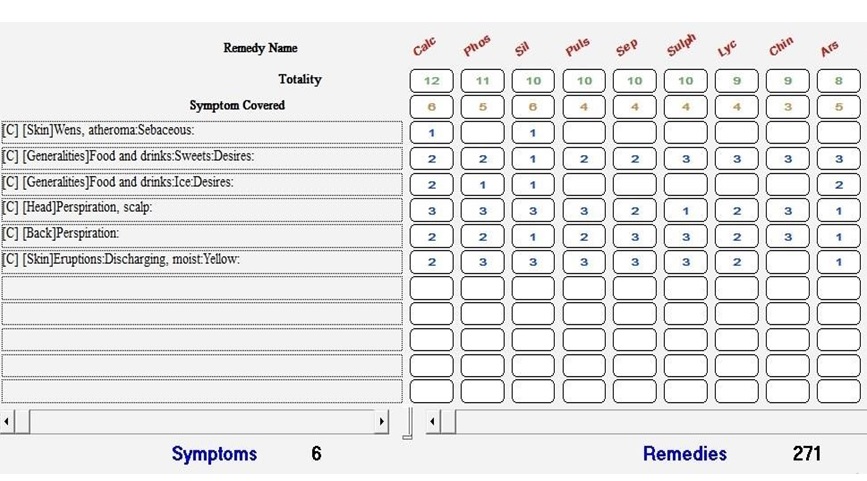
The following remedies rank high in the repertory sheet Calc (12/6)
Phos (11/5) Silicea (10/6) Puls (10/4) Sep (10/4)
Now as this case has very few characteristic symptoms to rely on, the pathological symptom or the pathology itself becomes an important differentiating factor. So if we see from that point of view the rubric –Skin – Wens, atheroma; Sebaceous is covered by only 2 of the top ranking remedies – Calcarea and Silicea
Now further going into differentiating between Calcarea and Silicea through Materia Medica[3] we find following points favouring Silicea over Calcarea
Silicea – Boericke’s Mm – Periodic states; abscesses;…SUPPURATIVE PROCESSES…Ripens abscesses since it promotes suppuration. Ailments attended with pus formation.
Final Prescription: Silicea 30 TDS x 4 days
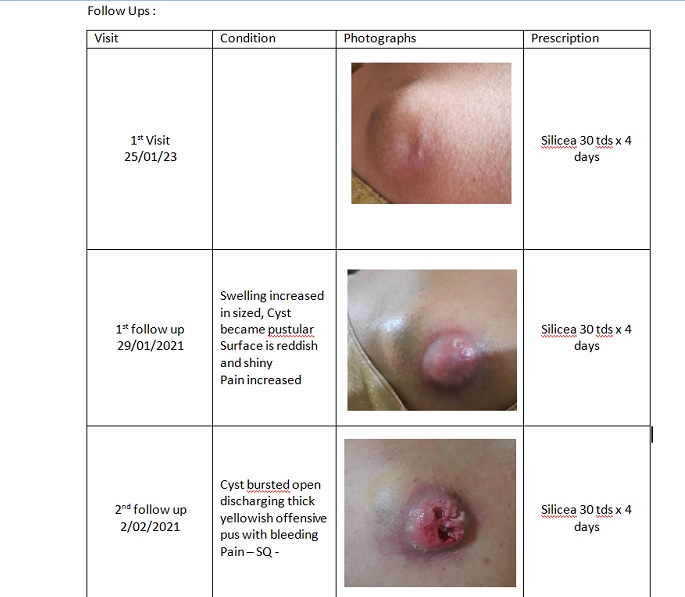
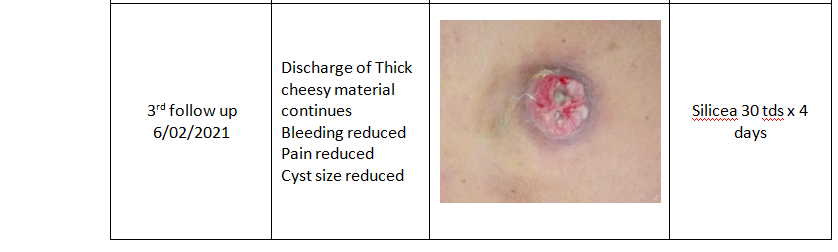
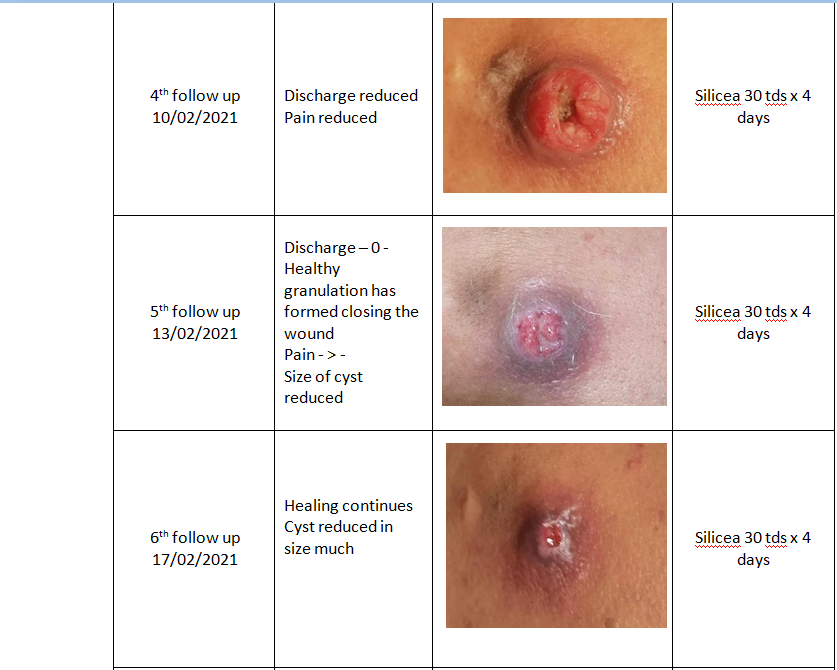
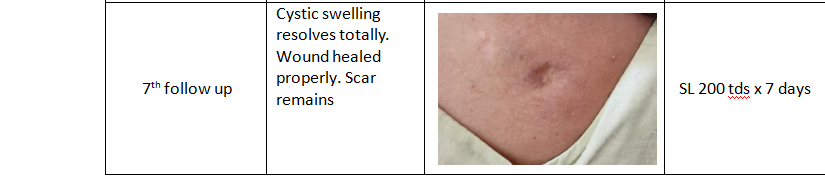
Follow Ups :
Discussion:
While treating
surgical one sided diseases or local diseases it is important to assess the
scope and limitations of treatment.
In the above case in discussion the patient had previously visited a surgeon and had her cyst drained but it kept
recurring. Here the underlying maism comes into play. While treating the patient homoeopathically it
is important to understand this deeper underlying cause of disease and to keep in mind the same while
selecting a suitable indicated remedy. For instance in this case as we see, that there is a tendency to recurrence of
symptoms, with pustular and cheesy necrotic discharges, the themes of Tubercular Maism come to mind. So while selecting a remedy it
becomes
important that we select a remedy which along with covering the totality also
belongs to Tubercular Maism.
Although this case falls under the category of chronic case, the presentation here is acute on chronic and hence it has been dealt in the same way. Lower potency of the indicated remedy with frequent repetition has been administered to take care of the acute inflammatory phase of the disease. Once this acute phase is settled it is important to follow up and administer a more suitable Constitutional Remedy to treat the more deep seated cause of the disease and thus prevent any recurrence.
This case highlights the efficacy
of Homoeopathic medicines in treating conditions, which would otherwise require surgical intervention,
effectively and safely. The saying that we all might have heard at some point as Silicea being
referred as the Homoeopaths Surgical Knife is aptly depicted by this case!
Bibliography:
- Neena Khanna, Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 4th Edition, Elsevier, 2011
- Ronald Marks, Roxburgh’s Skin Diseases, 17th edition, Arnold – Hodder Headline Group, 2003
- Samuel Hahnemann, Translated by William Boericke, Organon of Medicine, 6th Edition, B. Jain Publishers, 2013
- Boericke W, Boericke O, Pocket Manual of Homoeopathic Materia Medica Comprising of Characteristic and Guiding Symptoms of all Remedies (Clinical and Pathogenetic), 3rd Edition,
B. Jain Publishers, 2012
- Roger Van Zandvoort, Complete Repertory, 2019, Hompath Classic, Mind Technologies
Bibliography:
- Neena Khanna, Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 4th Edition, Elsevier, 2011
- Ronald Marks, Roxburgh’s Skin Diseases, 17th edition, Arnold – Hodder Headline Group, 2003
- Samuel Hahnemann, Translated by William Boericke, Organon of Medicine, 6th Edition, B. Jain Publishers, 2013
- Boericke W, Boericke O, Pocket Manual of Homoeopathic Materia Medica Comprising of Characteristic and Guiding Symptoms of all Remedies (Clinical and Pathogenetic), 3rd Edition,